Homoeopathy in Childhood Diarrhea Management Program
Tridibesh Tripathy
1
,
Prof. Shankar Das
2
,
Anjali Tripathy
3
,
Rakesh Dwivedi
4
,
Mohini Gautam
5
,
Sovesh Chandra Tripathy
6
1
BHMS (Utkal University, Bhubaneswar), MD (BFUHS, Faridkot), MHA (TISS, Mumbai), Ph.D. in Health Systems Studies (TISS, Mumbai), Homoeopathic & Public Health Expert, Subject Expert, Master of Public Health (Community Medicine) Program, Lucknow University, Lucknow, India
2
Dean, School of Health Systems Studies, Tata Institute of Social Sciences, Mumbai. Former Director, IIHMR, Delhi, India
3
Program Co-ordinator, Water Aid, UP office, Lucknow, India
4
Associate Professor, Centre for Advanced Studies in Social Work, Department of Social Work, Lucknow University, Lucknow, India
5
Assistant Professor, Centre for Advanced Studies in Social Work, Department of Social Work, Lucknow University, Lucknow, India
6
Proponent of Homoeopathy and Public Health, Employee, IB River Valley Coal Fields, Coal India Limited, Jharsuguda, Odisha, India
One of the most significant contributions of the Indian sub continent to the human kind is the gift of Oral Rehydration Therapy/Solution to deal with Cholera & other diarrheal diseases. The current article examines the contribution of Homoeopathy to deal with diarrheal diseases. The article traces the development of ORS both at global & the national level. Thereafter, it deals with the subject of diarrhoea through the dimension of how, why, when, where and whom of diarrhoea. Following that the burden of the disease as such is explained along with the intervention of OZ (ORS &Zinc) duo to deal with the disease. Interventions are also seen through the lens of prevention and protection as well. Taking cue from one of the elaborate & established books in the Homoeopathic world, it deals with what Homoeopathy had offered, is offering & the potential to offer in the future to deal with this water borne disease.
Keywords
Homoeopathy in Childhood Diarrhea Management Program
INTRODUCTION
In the past, in 1831 Homoeopathy was used successfully for Asiatic cholera. In the same period, there was a cholera epidemic in Vienna and Homoeopathy succeeded here as well. In another epidemic of cholera in 1846 in Europe, again Homoeopathy proved fruitful. However, one of the most successful effort was demonstrated in the 19th century cholera epidemic in London in 1854.
In the 20th century, it cared to mostly chronic diarrheal cases but again in 21st century, the gut bacteria has come to the lime light and it is here that Homoeopathy has again come in the fore front for diarrhea.
In the 21st century, with COVID 19 affecting the GI system in a great way, Homoeopathy has not only dealt the diarrhea symptom but also the whole issue of COVID 19. The major issue is that the treatment of diarrhea through Homoeopathy has not been reflected in large scale surveys like NFHS. Although in the NFHS 4 questionnaire, there is a section mentioning seeking treatment from a homoeopath for diarrhea, in the analysis of treatment, it is clubbed under the indicator ‘treated with home remedy/herbal/other’ & the report says that 12% of children with diarrhea were treated either with home remedy or herbal or others. It is in the others category homoeopathy is clubbed. Hypothetically, if we divide the response among the three options, it emerges that only 3% of children with diarrhea were treated homoeopathically either from private or public sector.
With this issue in the background, the current article examines what Homoeopathy can offer in the emerging & challenging nature of the enteric diseases and enteropathy.
Officially both Homoeopathy & ORS emerged in India in the late 1970s. Hence, it is wise to see the journey of homoeopathic treatment in diarrheal diseases in India as till date, they have travelled parallel. From 1980 to 2015, India achieved 86% reduction in number of deaths in U5 children due to diarrhea. Similarly, from 2.5 million diarrheal deaths in 2001, India reduced the number to 1.5 million. Unfortunately, there is no large scale survey to decipher the role of homoeopathy in the reduction of these deaths but what we have is only the number of users of homoeopathy in diarrhea without any follow up data. The current effort aims to suggest a treatment protocol as per the age categories of children till 5 years of age.
Histrory of Diarrhea & ORT
A group of physiologists observed that glucose enhances the absorption of sodium and water across the intestinal brush border membrane of experimental animals & that no morphological changes occur in the gut epithelium of Cholera patients. Cholera drove the sanitary revolution in the industrialized world in the 19th century and then drove the development of Oral Rehydration Therapy (ORT) in the developing world. Following the efforts of Captain Phillips, the Cholera research laboratory, Dhaka & the infectious diseases hospital, Calcutta developed the modern ORS. Similarly, the modern implementation of Oral Replacement Therapy was done by pediatricians in 1940 who used electrolyte solution as maintenance therapy in mildly purging children with diarrhea. Basic physiologic research in 1950s demonstrated the co-transport mechanism of sodium and organic solutes(sugars & amino acids) in the intestinal cells, there by establishing the scientific basis for ORT [1,2].
History of ORT at global level
The discovery that sodium transport and glucose transport are coupled in the small intestine so that glucose accelerates absorption of water and solute is potentially the important medical advance of this century [1,3-16].
Table 1 describes the time line towards development of ORT at the global level.
History of diarrhea program in India
Table 2 describes the time line of the progress of the diarrheal disease control program in India [7,17-18].
Table 1:
1940- Paediatricians used electrolyte solution as maintenance therapy in mildly purging children with diarrhea.
1964- Use of ORT based on scientific observations from Philippines by Captain Phillips of US army & Co-workers where they successfully tried glucose saline on two cholera patients.
1965-69- Efficacy of standard ORS demonstrated by Pierce, et.al & others.
1971-72- Dr. Dillip Mahalanabis showed efficacy of ORS in cholera cases among Bangladesh refugees.
1974- De et.al demonstrated the efficacy of ORS in children in diarrhea.
1978- Sircar et.al, demonstrated the efficacy of ORS in a cholera epidemic in Manipur.
1978- Chatterjee et.al, demonstrated the efficacy of ORS in children in diarrhea.
1978- WHO launched the global diarrhea disease control program with ORS at its heart and the short term objective of reducing mortality due to diarrhea.
1979- Dr. Daniel Pizarrow & colleagues showed efficacy of ORS in neonates.
1984- Dutta et.al & Roy et.al reported safety & simplicity of uninterrupted breast feeding.
Table 2:
1978- National diarrhea disease control program launched.
1985-86- National ORT program introduced.
1992- Diarrhea program became a part of Child Survival & Safe Motherhood Program (CSSM).
1997- CSSM became a part of Reproductive and Child Health program (RCH).
2003- Integrated Management of Neonatal and Childhood Illnesses (IMNCI) strategy became a part of RCH phase II program.
2005- Became a part of child health program and Childhood Diarrhea Management Program (CDMP) launched.
2006- Since November 2006, Zinc introduced in CDMP.
2013- RMNCH+A launched
2014- India Action Plan for Pneumonia & Diarrhea (IAPPD) launched following the Global Action Plan for Pneumonia & Diarrhea(GAPPD) launched by WHO in 2013.
2014- Intensified Diarrhea Control Fortnight (IDCF) launched as part of CDMP
About diarrhea
Diarrhea is defined as the passage of three or more loose or liquid stools per day (or more frequent passage than is normal for the individual). Frequent passing of formed stools is not diarrhea, nor is the passing of loose, pastry stools by breastfed babies [19].
Safe drinking water, use of improved sanitation, hand washing with soap reduces risk of diarrhea. Diarrhea is usually a symptom of an infection in the intestinal tract, which can be caused by a variety of bacterial, viral and parasitic organisms. Infection is spread through contaminated food or drinking water or from person-to-person as a result of poor hygiene.
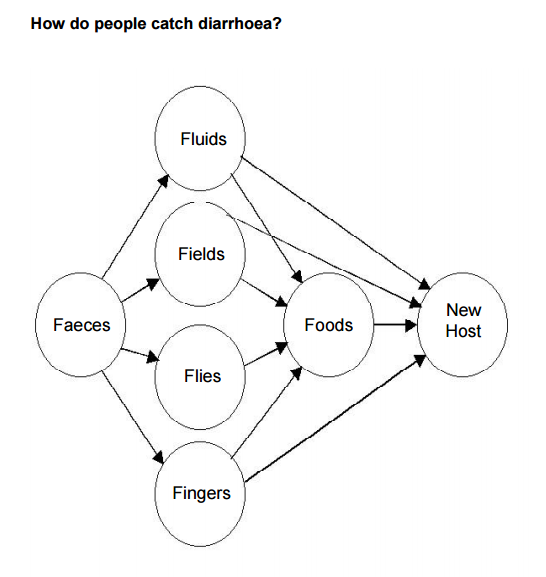
The following Figure 1 popularly called the F- diagram8 describes the Oro-Fecal route of transmission through the five Fs. Basically it describes the behaviors of the community regarding excreta disposal in rural areas & small communities. Through these behaviors, it describes how people catch diarrhea.
Typesof diarrhea
There are three types of diarrhea. These are acute watery diarrhea, acute bloody diarrhea & persistent diarrhea. Severe threat of diarrhea is dehydration [4,5].
Acute watery diarrhea lasts several hours to days & includes cholera.
Acute bloody diarrhea is also called dysentery.
Persistent diarrhea lasts 14 days or longer.
Pathology & Physiology of Diarrhea
Normal healthyintestine has numerous tiny hairs as ‘Villi’, the surface cells absorb metabolites from ingested food. There is a difference between the ce lls of the tips of the villi and the cells at the base. Rota virus strips the villi from large patches of intestine thus decreasing the surface area of absorption by 50% leading to mal-absorption [8].
Figure 1: How do people catch diarrhea?
Source- Wagner & Lanoix, WHO, 1958
Thus, in a child having diarrhea, first the sodium depletes and in chronic diarrhea potassium decrease leading to malnutrition and further diarrhea. In persistent diarrhea, loss of potassium leads to loss of muscle tone leading to a big abdomen.
Total body water is 42 liters where 25 liters is as intracellular fluid and the other 17 as extracellular that includes plasma, interstitial and trans-cellular fluids. Normally, 20 liters of water is secreted and the same is absorbed every day. This is how soluble metabolites from digested food is absorbed through blood stream. During diarrhea, this balance is upset and much water is lost than reabsorbed. With water, sodium is also lost. Kidneys maintain sodium normally. In dehydration due to diarrhea, anuria occurs because of which the sodium regulation cannot work. If more than 10% of body fluid is lost, death occurs. However, the current article does not deal in detail about dehydration.
About WASH34,35,36
Diarrhea comes under the Water, Sanitation & Hygiene (WASH) sector interventions of public health and comes under the domain of water borne diseases. Among Sustainable Development Goals (SDG), Goal #3 & 6 are related to good health, well being & drinking water, sanitation respectively. Agencies like WaterAid also works on WASH sector internationally since 1981 and in India since 1986 with the vision of ensuring a world where everyone has safe water, sanitation and hygiene. Currently, the Swachh Bharat Mission rolls out the interventions through the domain of WASH strategy.
About ORS16,17,13
Increased relative concentration of sodium across the intestinal wall pulls water through. We can see in the following table that the old formulation had both the chloride and bicarbonates of sodium. Further, we also see that in new formulation even if chloride of sodium is only 2.6 grams in comparison to 13.5 grams of glucose, their osmolarity is same in solution. This was not the case with the old formulation of ORS that was in use since 1978 till 2002 where the molarity of sodium was less than glucose leading to osmosis in the intestine. The new formulation came into use since 2002 that had the sodium & glucose in 1:1 ratio in solution. Starch like rice water is metabolized into glucose and it has less osmotic effect. This shows why rice water is still an effective home remedy in diarrhea. Citrate in new formulation is added to correct renal functions especially for infants. Thus, the new formulation prevents metabolic acidosis. Infants have large surface area of intestine, higher metabolic rate and underdeveloped renal function.
Table 3 compares WHO ORS old and new formulation in both dry powder form and in solution.
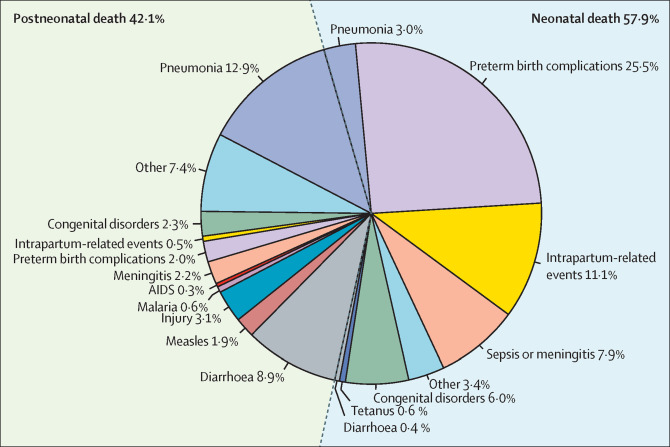
Burden of Diarrhea
As evident from the above figure, diarrhea causes 8.9% of all deaths from 1-59 months aged children in the under 5 group and 0.4% deaths in the 0-1 months aged children in the under 5 group. Thus, globally diarrhea accounts for 9.3% deaths among all the deaths among under 5 children. This data also holds good for India. The total number of live births in India as per census 2011 is 2% of 125 crore which is 2.5 crore. Further, the current U5 mortality rate of India is 34 per 1000 live births. Hence in 2.5 crore live births, there will be 8,50,000 deaths among U5 children in India in a year. Among these deaths, 9.3% are due to diarrhea in a year. Rounding up 9.3% to 10%, we see that 10% of 8,50,000 deaths or 85,000 deaths are due to diarrhea in India in a year.
Besides these number of deaths, the report of National Commission on Macroeconomics & Health in 2005 estimated that diarrheal episodes per year among U6 is 760 per lakhs and it was projected that in 2015, the episodes will be 880 lakhs per year. Similarly, the average estimated incidence of diarrhea in U6 children was 1.71 and 1.09 episodes per person per year in rural & urban areas respectively. This data of 1.7 episodes of diarrhea was used by state governments to plan their diarrhea programs for U5 till 2012. The team of Fischer Walker in 2012 estimated that the incidence of diarrhea has declined from 3.4 episodes per child per year in 1990 to 2.9 episodes per child per year in 2010. Among infants aged 6-11 months of age, it was 4.5 episodes per child per year in 2010.
Table 3:
Old formulation of ORS
New formulation of ORS
ORS dry powder form- 27.5 grams in total
-Sodium Chloride- 3.5 grams
-Sodium Bicarbonate-2.5 grams
- Potassium Chloride- 1.5 grams
- Glucose- 20grams
ORS dry powder form- 20.5 grams in total
-Sodium Chloride- 2.6 grams
- Sodium Bicarbonate-0 grams
- Potassium Chloride- 1.5 grams
- Sodium Citrate- 2.9 grams
- Glucose- 13.5 grams
ORS in solution- Osmo-molarity of components- 341mmol/l in total
Glucose- 111
Sodium-(Na+)-90
Potassium-(K+)-20
Chloride-(Cl-)-80
Bicarbonate-(HCO3)- 30
ORS in solution- Osmo-molarity of components- 245mmol/l in total
Glucose- 75
Sodium-(Na+)-75
Potassium-(K+)-20
Chloride-(Cl-)-65
Citrate-10
Figure 2: Source- Liu L et.al, 2019
Current Situation of Diarrhea in India
The current situation of diarrhea can be best seen from the cross sectional survey on diarrhea through the National Family Health Surveys. The table 4 shows the details of diarrhea related indicators from NFHS 1 to NFHS 5. It is to be noted that in the first two rounds, there was no data on zinc as it was not introduced at that time. The latest data is from NFHS 5 which was released in November 2021. In comparison to NFHS 4, in NFHS 5, we can see the drop in the prevalence rate is 1.9% where as there is 10% increase in ORS uptake and 10.2% increase in Zinc uptake in children having diarrhea [9-11,18-20].
Dealing with Diarrhea
Diarrhea was dealt with only ORS since 1978 in India and it was in 2005 when NRHM was launched, Zinc was introduced along with ORS. The Protection, Prevention and Treatment (PPT) model is adopted to deal with diarrhea. Table 4 details out the models [4,5,13-15].
Rota virus vaccination
Rota virus is responsible for 60% of all diarrheal cases in children. At global level & in India, Rotashield (Wyeth-Lederle vaccines) vaccination was launched by WHO in 1998. The other two Rota virus vaccines were Rotarix (Glaxosmithkline) and Rotateq (Merck) showed complication in the form of intussusceptions of the intestines. Rotarix was a monovalent human rota virus vaccine & Rotateq was a pentavalent bovine-human vaccine. Majority of the complications were with Rotashield with few cases in the other two. Government of India launched Rotavac vaccine of Bharat Biotech of India in the Universal Immunization Program in 2016. It was not associated with any complications. Rotavac is an oral monovalent, live, attenuated vaccine that contains Bovine-Human reassortment 116E strain. The vaccine is administered through 3 doses at 6, 10 & 14 weeks of age.
The NFHS 5 report mentions that 36.4% children aged 12-23 months have received 3 doses of Rotavirus vaccine.
Example of a work load of ASHA regarding diarrhea
On an average, An Accredited Social Health Activist (ASHA) covers 1000 population which means there are 150 U5 children in her catchment area as 15% of population constitutes U5 children. Taking into account the average number of episodes per child per year which is 2.9 times, we find there will be 450 episodes of diarrhea among U5 children in her area in a year. Usually, a diarrheal episode subsides with 2 packets of ORS per child on an average. So the ASHA will need 900 ORS packets in a year and 7300 Zinc tablets in a year considering 14 tablets per episode. Here, we have to see that not all cases will report to ASHA or the public health system. For example, the Health Management Information System of Government of UP informs that only 25% of cases report to the public health system. Hence, the ASHA will be given 250 packets of ORS & 1825 Zinc tablets in a year. The majority of the supply i.e. 75% of these ORS & Zinc tablets will be given to ASHA during April to September when the diarrheal episodes are at peak in the community. This is the seasonal trend as per the science of epidemiology [7,9,10,14,19-22].
IDCF- a Campaign & a Movement
Government of India introduced the Intensified Diarrhea Control Fortnight in 2014 where the last week of July month & the first week of August were clubbed to celebrate the fortnight. National ORS day falls on July 29. The first week of August is known as World Breastfeeding Week (WBF). In the first week, the ASHA is supposed to distribute two packets of ORS to every child U5 so that they are given ORS in case they suffer from diarrhea during this peak season of diarrhea. She is supposed to give 14 tablets of Zinc to every case of diarrhea in her catchment area. In the second week, she has to identify 0-2 year old children so that the concepts of breast feeding and complementary feeding practices are reinforced to the mothers of these children. As these are integral part of WBF, this practice is critical in the second week. At the institutional level, OZ corners are set up at CHC, PHC, DH & state level hospitals to reinforce the use of OZ in diarrhea. Every year, these two week campaigns across the state, district & blocks lead to the uptake & use of OZ in diarrhea. At the end of the campaign, reports are sent by the state to the centre that includes details of activities like training, IEC materials, symposiums, workshops at all levels [31-38].
Concept of essential medicine
The National List of Essential Medicine (NLEM) mentions OZ as essential medicines. An essential medicine has to have three qualities which are effectiveness clinically, cost effective and should not have side effects. OZ meets all the three criteria. It is clinically effective and does not have side effects. As an example, the Government of UP buys one ORS packet for ₹2 and one tablet of Zinc costs 14 paise. On an average, a child recovers in 2 days which means ₹4 is spent for ORS in an episode of diarrhea. Similarly, ₹1.96 or ₹2 is spent on 14 tablets of Zinc for an episode. So in all, ₹6 is spent on each episode. This demonstrates that OZ is cost effective as well. It is also used at all the three levels of care viz. Primary, Secondary & Tertiary (PST) so that all the prescribers at these levels develop the habit of prescribing OZ [5,23,24].
Three compounds of Zinc are used as supplements for diarrhea. These are Zinc Sulphate, Zinc Gluconate & Zinc Acetate. Although Zinc Acetate is best absorbed, the public health system uses Zinc Sulphate as it is cheap among the three compounds.
Zinc & Nutrition
Zinc supplementation in infants and early childhood but not on pregnancy increases specific growth outcomes, with evidence for a potentially stronger effect after 2 years of age. Zinc is lost through stools in diarrhea and it is an essential micronutrient that builds T immunity cells through the stimulation of Thymus gland till adolescence after which thymus becomes dormant. Hence, Zinc supplementation is critical in diarrhea in U5 children. Zinc as a micronutrient is also related to stunting in U5 children if there is a deficiency of Zinc in children less than 5 years of age. A dose regimen of 14 days of zinc completes the need for children for a year. The need of zinc is further felt when we see that as per the incomplete data in NFHS 5, 2019-20, in 13 out of 22 states, the rate of stunting has increased in comparison to NFHS 4, 2005-06 with Gujarat leading the list with 39% stunted children. Stunting which is low height for age is categorized as chronic malnutrition. Vegetarians are further devoid of Zinc as the major sources are the non-vegetarian foods. Thus, the zinc supplementation becomes critical for all children [4,5,6,25].
Homoeopathic approach- Current situation
The Essential Drug List (EDL) of Homoeopathy mentions Gastro Intestinal disorder as one of the many disorders for which a list of 233 medicines besides the 12 biochemics, ointments & drops. The preferred potencies of the 233 medicines are only color coded with a color index. There is no clarity for which the medicine is to be given. It is highly vague & broad [39,40].
Another document in the public domain is the 7th training module of ASHAs where a few homoeopathic medicines are mentioned against their therapeutic uses for the dissemination of the information by ASHAs at the community level. The drug kit supplied to ASHA by the states does not have homoeopathic medicines [39-40].
Homoeopathic approach- a new dimension
The current article does not try to repeat the Materia Medica related to diarrhea therapeutics. Instead, it approaches Homoeopathy through the eyes of the PPT model discussed above. Please note that ORS to be given in all cases as per the dose according to the age that is mentioned on the ORS packets. ORS is to be given till the diarrhea lasts [37,41].
For newborn (0-28 days old child)- Prescribe Colostrum in potency in repeated doses. Specifically prescribe Colostrum for all newborns who did not receive colostrums in their first three days of life. As we know, all potencies are immune boosters. Breast feeding to be continued optimally as usual. Zinc is not to given for less than 2 months old child. Hence, it is better to avoid Zinc based homoeopathic triturations during this stage.
For 1-5 months old or 0-6 months old- Prescribe Lac Humanum, Lac Materna, Lac Vaccini Flos. These are prepared from human breast milk only. Lac Vaccini Flos will develop brown fat in the neonant since it is prepared from cream. It is not white fat but the brown fat that protects the child from hypothermia & the related electrolyte imbalances because of diarrhea. Since this is the time when only mother’s milk is to be given & even water is not be given. Besides mother’s milk, only oral vaccines, ORS & prescribed medicines are allowed as per the concept of Exclusive Breast Feeding (EBF). During treatment, breast feeding to be continued optimally as usual. Here, we can prescribe Zincum Met-3X, one tablet powdered and put in a tea spoon of mother’s milk & give once a day for 14 days. We can also prescribe Zinc Sulph or Zinc Acetate in potency in repeated doses till the diarrhea stops. As mentioned above, Zinc sulphate, Zinc acetate & Zinc gluconate are given to children in the diarrhea management program. Homoeopathy does not have any medicine prepared from Zinc gluconate.
For 6-23 months old or children under 2 years of age- Breast feeding & home-made complemeiven as weaning practices. Since at this time, we need to complete the need, from 6-12 months old child, breast feeding to be reduced to 50% and the other 50% needs to come from home made complementary foods. Similarly, for 12-24 months, breast feeding to fulfill 25% need & the other 75% to come from home made complementary foods. Here we can add Zincum Met-3X, Zinc Acetate or Sulphate in potency. Along with that, we can add Natrum Mur-3X since the dry ORS has sodium chloride.
For 2-5 year old- Complete diet including cereals, pulses, green vegetables, green leafy vegetables & fruits. No Breast Feeding is to be given in this age as breast feeding is up to 2 years of age only. Along with Zincum Met-3X, prescribe Zinc sulphate or Zinc acetate in potency. Along with Natrum Mur-3X, we can add Kali Chlor in potency since ORS in dry form has Potassium Chloride as a constituent.
Homoeopathy has 13 medicines prepared from Zinc compounds or the metal itself. These are zinc aceticum, zinc arsenicosum, zinc bromatum, zinc chromatum, zinc cyanatum, zinc iodatum, zinc metallicum, zinc muriaticum, zinc oxydatum, zinc phos, zinc picric, zinc sulph & zinc valeriana. Since metallic zinc is useful in diarrhea, we can delve in to these short acting zinc compounds & prescribe in cases of diarrhea [37-41].
Table 4:
NFHS 1- 92-93
Indicator-Percentage of children suffering from diarrhea in previous 2 weeks-‘Any’ diarrhea- 10
Bloody diarrhea-1.3
-Any diarrhea in previous 24 hours-4.8
-Knowledge about ORS packets- 42.7
-Have ever used ORS packets-25.9
NFHS 2- 1998-99
Indicator- Percentage of children less than 3 years of age who reported diarrhea in the preceding 2 weeks – 19.2
-Percentage of 1-35 months old children with diarrhea who received ORS-26.8
NFHS 3-2005-2006
Indicator- Percentage of children less than 5 years of age who were suffering from diarrhea in last 2 weeks- 9.
-Percentage of children with diarrhea who received ORS-26
-Percentage of children with diarrhea who received Zinc-not available
NFHS 4- 2015-16
Indicator- Prevalence of diarrhea (reported) in the last two weeks preceding the survey (%)-9.2
-Percentage of children with diarrhea who received ORS-50.6
-Percentage of children with diarrhea who received Zinc-20.3
NFHS 5-2019-2021
Indicator- Prevalence of diarrhea (reported) in the last two weeks preceding the survey (%)-7.3
-Percentage of children with diarrhea who received ORS-60.6
-Percentage of children with diarrhea who received Zinc-30.5
Table 5:
Protection
Colostrum feeding (Early Initiation of Breast Feeding)
Exclusive Breast Feeding from 0-6 months of age (allowed substances are oral vaccines, ORS & prescribed medicines)
Infant & Young Child Feeding (IYCF) that includes Complementary feeding along with breast feeding for 6months to 2 years old children.
Balanced diet that includes cereals, pulses, green vegetables, green leafy vegetables, fruits, dairy products and non-vegetarian foods for 2-5 year old children.
Prevention
Hand washing with soap before 7 critical action points
Clean drinking water
Use of functional toilets
Rota virus vaccination
Treatment
ORS till the diarrhea stops
Zinc supplementation for children above 2months. Zinc 10mg dispersible tablet once a day for 2-6 months old children with mother’s milk for 14 days even if the diarrhea has stopped.
For 6 months to 5year olds, 20 mg dispersible zinc tablet with milk or water once a day for 14 days even if the diarrhea has stopped.
In case of dysentery, the prescribers can add ‘Mercurius Corrosivus’ as a specific in potencies along with the above medicines. Similarly in case of persistent diarrhea, ‘China’ in potencies can be prescribed as a specific owing to the loss of vital fluids through the electrolyte losses in chronic diarrhea.
Taking cue from the program related interventions & the use of OZ, the above prescriptions are based on ‘Tautopathic’ method of prescription in homoeopathy. These zinc based medicines will also prevent the child from ‘stunting’, low height for age phenomenon which is a manifestation of chronic malnutrition. The importance of the issue of stunting is mentioned in detail in asection above in this article. Zincum Met 3X will also stimulate the Thymus gland to produce optimum amount of T cells of the immune system as it contains small amounts of elemental Zinc.
CONCLUSION
Many Homoeopaths may not agree to the concept mentioned above. The point is if targeted & homoeopathic approaches are not followed in dealing with issues of public health that aims to reduce mortality & morbidity, homoeopathy will lag behind. The homoeopathic fraternity has to adhere to the program guidelines of various ongoing programs to allow homoeopathy to come to the limelight. Currently, many homoeopaths are working as third medical officers on contractual basis under NHM at the district & block level but they do not use homoeopathy at all. They simply adhere to their routine work & in the process have forgotten homoeopathy completely. Conventional homoeopathy is OK in private practice & in educational institutions but when you want to address masses; homoeopathy has to complement the existing program roll out. Diarrhea is still a major killer of U5 children in India currently. Adhering to the new approach will only strengthen homoeopathic system of therapeutics in the long run.
Declaration
The authors declare that there was no funding received for this article. Professor Shankar Das, a co-author of this article was the Ph.D. guide of the lead author of this article at Tata Institute of Social Sciences, Mumbai. The lead author thanks all the co-authors for their input in the non-homoeopathic section of the article. The lead author declares that the homoeopathic section is only suggestive in nature.
Conflict of interest
There is no conflict of interest regarding this article.
REFERENCE
Bhattacharya, S.K. "History of Development of Oral Rehydration Therapy." Indian Journal of Public Health, vol. 38, no. 2, Apr.–June 1994, pp. 39–43.
Guerrant, R.L., et al. "Cholera, Diarrhea & ORT: Triumph & Indictment." Journal of Clinical Infectious Diseases, vol. 37, no. 3, Aug. 2003, pp. 398–405. DOI: 10.1086/376619.
Da Cunha, R.M., and R.A. Cash. "History of Development of Oral Rehydration Therapy." Journal of Clinical Therapeutics, vol. 12, suppl. A, 1990, pp. 2–11.
World Health Organization. "Diarrhoea Disease." 2017, www.who.int/news-room/fact-sheets/detail/diarrhoea-disease.
World Health Organization. Ending Preventable Deaths from Pneumonia and Diarrhoea by 2025. Apr. 2013.
National Family Health Survey (NFHS), 2, 3, 4, and 5. International Institute for Population Sciences (IIPS), Mumbai.
Ministry of Health and Family Welfare, Government of India. Guidelines on CDMP. 2013.
Wagner, Edmund Glen, Joseph Nicker, and WHO. Excreta Disposal for Rural Areas and Small Communities. 1958, WHO Monograph Series No. 39, ISBN 9241400390, https://apps.who.int/iris/handle/10665/41687.
Fischer Walker, Christa L., et al. "Diarrhoeal Diseases Among Children." BMC Public Health, vol. 12, no. 220, 2012, https://doi.org/10.1186/1471-2458-12-220.
Government of India, Ministry of Health and Family Welfare. Report on National Commission on Macroeconomics and Health, Disease Burden Estimation. Aug. 2005.
Liu, L., et al. "National, Regional, and State-Level All-Causes and Cause-Specific Under-5 Mortality in India in 2000–2015: A Systematic Analysis with Implications for the SDGs." The Lancet Global Health, vol. 7, June 2019, https://doi.org/10.1016/s2214-109x(19)30080-4.
Government of India, Ministry of Health and Family Welfare. India Newborn Action Plan. Sept. 2014, https://nhm.gov.in.
Bhatnagar, S., et al. "IAP Guidelines 2006 on Management of Acute Diarrhea." Indian Paediatrics, vol. 44, 2007, pp. 380–89.
Government of India, Ministry of Health and Family Welfare. Use of Zinc as an Alternate Therapy in the Treatment of Diarrhea. Department of Family Welfare, Child Health Division, No. Z-28020/06/2005-CH.
Government of India, Press Information Bureau. Action Plan Against Pneumonia and Diarrhea. 24 Feb. 2015.
Goodall, R.M. "Oral Rehydration Therapy: How It Works." The Lancet, 5 Aug. 1978, www.rehydrate.org/ors-how-it-works.htm.
World Health Organization. "New Formula Oral Rehydration Salts." WHO Drug Information, vol. 16, no. 2, 2002, www.rehydrate.org/newformula-studies.html.
World Health Organization, UNICEF, and World Bank. Mortality Estimates, Population Division of United Nations, Department of Economic and Social Affairs. 2019.
Government of India, Registrar General of India. Census of India, 2011.
Government of Uttar Pradesh, National Health Mission. PIP 2005–06, Child Health Section on Diarrhea. 2006.
Government of Uttar Pradesh, National Health Mission. HMIS, Child Health Section. 2005–2006.
Singh, M., and S. Saini. Conceptual Review of Preventive & Social Medicine. 2nd ed., CBS Publishers & Distributors Pvt Ltd, 2019–2020, ISBN 978-93-88725-84-2.
Government of India, National Health Mission. NLEM, Free Drugs. 1 Oct. 2021, https://www.nlm.gov.in.
Government of Uttar Pradesh, Directorate of Medical and Health Welfare. Drug Procurement Division. Swasthya Bhawan, Lucknow, 2006.
Liu, E., et al. "Effect of Zinc Supplementation on Growth Outcomes in Under-5 Children." Nutrients, vol. 10, no. 3, Mar. 2018, p. 377, https://doi.org/10.3390/nu10030377.
Leary, B. "Oral Rehydration Therapy and Gastrointestinal History." Med Ges Gesch, vol. 16, 1997, pp. 125–44, pubmed.ncbi.nih.gov/11623647.
Venkat Homoeo. "A Review on Epidemic Success of Homoeopathy." 2021, venkathomeo.org/archives/vhmcarticles/article-006.
Moise, Ana Maria R. The Gut Microbiome. Greenwood Publishing Group Inc., 2021, ISBN 9781440842641.
Tripathy, T., et al. "Homoeopathy in COVID-19: A Treatment Protocol for Second and Third Wave." Scholars International Journal of Traditional and Complementary Medicine, vol. 4, no. 6, 2021, pp. 86–90.
Tripathy, T., et al. "Homoeopathy in COVID-19: A Multi-Stage and Multi-Dimensional Approach." European Journal of Biomedical and Pharmaceutical Sciences, vol. 7, no. 5, 2021, pp. 263–66, ISSN 2349-8870.
Subitha, L., and J. Ramakrishnan. "Diarrheal Diseases Among Children in India: Current Scenario and Future Perspectives." Journal of Natural Science, Biology and Medicine, vol. 6, no. 1, Jan.–June 2015, pp. 24–28.
Choudhary, T.S., et al. "Factors Associated with the Decline in Under-5 Diarrhea Mortality in India: A List Analysis." Journal of Global Health, vol. 9, no. 2, 22 Oct. 2019, p. 020804.
Reddy, S.N., et al. "Intussusception After Rotavirus Vaccine Introduction in India." New England Journal of Medicine, vol. 383, 2020, pp. 1932–40.
United Nations. Sustainable Development Goals. Passed in UNGA, Sept. 14, for the Period of 2015–30.
Government of India, Ministry of Drinking Water and Sanitation. Swachh Bharat Mission Guidelines. Oct. 2014.
Murphy, Robin. Lotus Materia Medica. B. Jain Publishers Private Limited, 6th impression, 2017, ISBN 978-81-319-0859-4.
Government of India, National Health Mission. IDCF Guidelines. Child Health Division, 2014, https://www.nrhm.gov.in.
Government of India, AYUSH. Essential Drug List, Homoeopathy. Department of AYUSH, Drug Control Cell, Ministry of Health and Family Welfare, Mar. 2013, www.indianmedicine.nic.in.
Government of India, National Health Systems Resource Centre. Induction Training Modules for ASHA. 2005.
Government of India, National Neonatology Forum. IAP, Ministry of Health and Family Welfare. 2014.
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Community Medicine and Public Health open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Recommended Articles
Research Article
Etiological Analysis of the Incident of Computer Vision Syndrome (Cvs) in Students of the Faculty of Medical Muhammadiyah University Semarang
Anang Kriswantoro,
...
Swasty
Published: 20/01/2026
Download PDF
Cite
x
APA
Kriswantoro, A., Martiningsih, W. R., Novitasari, A. & None, S. (2026). Etiological Analysis of the Incident of Computer Vision Syndrome (Cvs) in Students of the Faculty of Medical Muhammadiyah University Semarang. Himalayan Journal of Community Medicine and Public Health, 7(1), 1-5.
MLA
Kriswantoro, Anang, et al. "Etiological Analysis of the Incident of Computer Vision Syndrome (Cvs) in Students of the Faculty of Medical Muhammadiyah University Semarang." Himalayan Journal of Community Medicine and Public Health 7.1 (2026): 1-5.
Chicago
Kriswantoro, Anang, Wahju R. Martiningsih, Andra Novitasari and Swasty . "Etiological Analysis of the Incident of Computer Vision Syndrome (Cvs) in Students of the Faculty of Medical Muhammadiyah University Semarang." Himalayan Journal of Community Medicine and Public Health 7, no. 1 (2026): 1-5.
Harvard
Kriswantoro, A., Martiningsih, W. R., Novitasari, A. and None, S. (2026) 'Etiological Analysis of the Incident of Computer Vision Syndrome (Cvs) in Students of the Faculty of Medical Muhammadiyah University Semarang' Himalayan Journal of Community Medicine and Public Health 7(1), pp. 1-5.
Vancouver
Kriswantoro A, Martiningsih WR, Novitasari A, Swasty S. Etiological Analysis of the Incident of Computer Vision Syndrome (Cvs) in Students of the Faculty of Medical Muhammadiyah University Semarang. Himalayan Journal of Community Medicine and Public Health. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Curves of Concern: Public Awareness of Scoliosis and Its Impact on Childhood Development in Hamirpur
Vishal Dhatwalia,
Swati Chandel
Published: 10/12/2024
Download PDF
Cite
x
APA
Dhatwalia, V. & Chandel, S. (2024). Curves of Concern: Public Awareness of Scoliosis and Its Impact on Childhood Development in Hamirpur. Himalayan Journal of Community Medicine and Public Health, 5(2), 1-6.
MLA
Dhatwalia, Vishal and Swati Chandel. "Curves of Concern: Public Awareness of Scoliosis and Its Impact on Childhood Development in Hamirpur." Himalayan Journal of Community Medicine and Public Health 5.2 (2024): 1-6.
Chicago
Dhatwalia, Vishal and Swati Chandel. "Curves of Concern: Public Awareness of Scoliosis and Its Impact on Childhood Development in Hamirpur." Himalayan Journal of Community Medicine and Public Health 5, no. 2 (2024): 1-6.
Harvard
Dhatwalia, V. and Chandel, S. (2024) 'Curves of Concern: Public Awareness of Scoliosis and Its Impact on Childhood Development in Hamirpur' Himalayan Journal of Community Medicine and Public Health 5(2), pp. 1-6.
Vancouver
Dhatwalia V, Chandel S. Curves of Concern: Public Awareness of Scoliosis and Its Impact on Childhood Development in Hamirpur. Himalayan Journal of Community Medicine and Public Health. 2024 Jul;5(2):1-6.
Download PDF
Research Article
Otolaryngologic Perspective on Endoscopic Sellar Reconstruction after Transsphenoidal Pituitary Surgery
Sattar Jaber Abed,
...
Asaad Mezher Hussain
Published: 31/12/2025
Download PDF
Cite
x
APA
Jaber Abed, S., Khazaal Hashim, M. & Mezher Hussain, A. (2025). Otolaryngologic Perspective on Endoscopic Sellar Reconstruction after Transsphenoidal Pituitary Surgery. Himalayan Journal of Community Medicine and Public Health, 6(2), 1-5.
MLA
Jaber Abed, Sattar, Mohammed Khazaal Hashim and Asaad Mezher Hussain. "Otolaryngologic Perspective on Endoscopic Sellar Reconstruction after Transsphenoidal Pituitary Surgery." Himalayan Journal of Community Medicine and Public Health 6.2 (2025): 1-5.
Chicago
Jaber Abed, Sattar, Mohammed Khazaal Hashim and Asaad Mezher Hussain. "Otolaryngologic Perspective on Endoscopic Sellar Reconstruction after Transsphenoidal Pituitary Surgery." Himalayan Journal of Community Medicine and Public Health 6, no. 2 (2025): 1-5.
Harvard
Jaber Abed, S., Khazaal Hashim, M. and Mezher Hussain, A. (2025) 'Otolaryngologic Perspective on Endoscopic Sellar Reconstruction after Transsphenoidal Pituitary Surgery' Himalayan Journal of Community Medicine and Public Health 6(2), pp. 1-5.
Vancouver
Jaber Abed S, Khazaal Hashim M, Mezher Hussain A. Otolaryngologic Perspective on Endoscopic Sellar Reconstruction after Transsphenoidal Pituitary Surgery. Himalayan Journal of Community Medicine and Public Health. 2025 Jul;6(2):1-5.
Download PDF
Research Article
Complications of Perianal Tuberculosis and Efficacy of Surgical Intervention: A Detailed Analysis
Karen Kallás Pinto,
...
Maristela Melhem Natrielli De Almeida
Published: 28/02/2026
Download PDF
Cite
x
APA
Pinto, K. K., Vilela de Oliveira, I. S. & De Almeida, M. M. N. (2026). Complications of Perianal Tuberculosis and Efficacy of Surgical Intervention: A Detailed Analysis. Himalayan Journal of Community Medicine and Public Health, 7(1), 1-5.
MLA
Pinto, Karen K., Isabella S. Vilela de Oliveira and Maristela M. N. De Almeida. "Complications of Perianal Tuberculosis and Efficacy of Surgical Intervention: A Detailed Analysis." Himalayan Journal of Community Medicine and Public Health 7.1 (2026): 1-5.
Chicago
Pinto, Karen K., Isabella S. Vilela de Oliveira and Maristela M. N. De Almeida. "Complications of Perianal Tuberculosis and Efficacy of Surgical Intervention: A Detailed Analysis." Himalayan Journal of Community Medicine and Public Health 7, no. 1 (2026): 1-5.
Harvard
Pinto, K. K., Vilela de Oliveira, I. S. and De Almeida, M. M. N. (2026) 'Complications of Perianal Tuberculosis and Efficacy of Surgical Intervention: A Detailed Analysis' Himalayan Journal of Community Medicine and Public Health 7(1), pp. 1-5.
Vancouver
Pinto KK, Vilela de Oliveira IS, De Almeida MMN. Complications of Perianal Tuberculosis and Efficacy of Surgical Intervention: A Detailed Analysis. Himalayan Journal of Community Medicine and Public Health. 2026 Jan;7(1):1-5.
Tripathy, T., Shankar Das, P., Tripathy, A., Dwivedi, R., Gautam, M. & Chandra Tripathy, S. (2021). Homoeopathy in Childhood Diarrhea Management Program. Himalayan Journal of Community Medicine and Public Health, 2(2), 1-8.
MLA
Tripathy, Tridibesh, et al. "Homoeopathy in Childhood Diarrhea Management Program." Himalayan Journal of Community Medicine and Public Health 2.2 (2021): 1-8.
Chicago
Tripathy, Tridibesh, Prof. Shankar Das, Anjali Tripathy, Rakesh Dwivedi, Mohini Gautam and Sovesh Chandra Tripathy. "Homoeopathy in Childhood Diarrhea Management Program." Himalayan Journal of Community Medicine and Public Health 2, no. 2 (2021): 1-8.
Harvard
Tripathy, T., Shankar Das, P., Tripathy, A., Dwivedi, R., Gautam, M. and Chandra Tripathy, S. (2021) 'Homoeopathy in Childhood Diarrhea Management Program' Himalayan Journal of Community Medicine and Public Health 2(2), pp. 1-8.
Vancouver
Tripathy T, Shankar Das P, Tripathy A, Dwivedi R, Gautam M, Chandra Tripathy S. Homoeopathy in Childhood Diarrhea Management Program. Himalayan Journal of Community Medicine and Public Health. 2021 Jul;2(2):1-8.