Xeroderma pigmentosum (XP) is a rare autosomal recessive disorder characterized by heightened sensitivity to ultraviolet radiation due to a deficiency in the endonuclease enzyme responsible for DNA repair. Aim: The study aimed to evaluate the role of chemical peels in clearing the skin background in patients with XP and reducing the rate of new lesion development.Patients and Methods: This study included 14 patients with XP, consisting of 9 males and 5 females, who underwent facial chemical peels using 30% trichloroacetic acid. The study was conducted between March 2011 and May 2012 at Al-Jamhouri Teaching Hospital in Mosul. Evaluation of results was performed by two plastic surgeons and patient satisfaction. Results: All patients underwent trichloroacetic acid peeling of the entire face, with the number of sessions varying. Specifically, one patient received 3 sessions, another patient received 4 sessions, and one patient received 6 sessions. Eight patients underwent 5 sessions, and three patients received 7 sessions of chemical peels. Patient and parent satisfaction was assessed, with 7 patients reporting high satisfaction and 7 patients indicating moderate satisfaction. Evaluation by two plastic surgeons revealed good results in 5 patients, moderate results in 7 patients, and poor results in 2 patients. Conclusion: Chemical peels offer a simple, well-tolerated procedure that effectively clears skin background changes and eliminates subclinical premalignant lesions, as diagnosed by fine needle aspiration cytology (FNAC). This procedure exhibits a prophylactic effect in XP patients and yields positive outcomes with minimal complications.
Keywords
Xeroderma pigmentosum
Chemical peels
Trichloroacetic acid
DNA repair
Patient satisfaction
Fine needle aspiration cytology
Prophylactic effect.
Important Note
Key findings:
The study evaluated 14 XP patients treated with 30% trichloroacetic acid peels. Patients underwent varying numbers of sessions. Patient and parent satisfaction was moderate to high. Plastic surgeons rated results as good in 5 patients, moderate in 7, and poor in 2. Chemical peels effectively cleared skin changes and reduced new lesion development.
What is known and what is new?
Xeroderma pigmentosum (XP) is a rare genetic disorder characterized by extreme sensitivity to ultraviolet (UV) rays due to a deficiency in DNA repair enzymes, leading to skin changes and an increased risk of skin cancer. This study evaluates the use of chemical peels, specifically 30% trichloroacetic acid, in XP patients to clear skin background changes and reduce the development of new lesions. The results suggest that chemical peels can be effective in managing XP-related skin issues and may have a prophylactic effect against skin cancer.
What is the implication, and what should change now?
Implication is the study suggests that chemical peels could be a beneficial treatment option for managing skin changes in XP patients and reducing the risk of new lesion development. Healthcare providers should consider incorporating chemical peels into the treatment plan for XP patients to help clear skin background changes and potentially reduce the risk of skin cancer. Further research and clinical trials could help establish guidelines for the use of chemical peels in XP management.
Introduction
XP is an autosomal recessive disease in which the individual is unable to repair the DNA damage caused by ultraviolet light .There is extreme photosensitivity of the skin and eyes with premature cutaneous aging and a 1000 fold increased frequency of cutaneous basal cell carcinoma, squamous cell carcinoma and malignant melanoma. XP is one of the families of diseases collectively termed as "the chromosome breaking syndromes" or "the DNA repairing disorder". This group includes Fanconi anaemia, ataxia-telangectasia, Blome syndrome, Cockayne syndrome and trichothiodystrophy. [1] XP was first described by Hebra and Kaposi in 1874. The disease was first called xeroderma or parchment skin. Later on the term pigmentosum was added to emphasize the striking pigmentary changes [2].The Italian physician Carlo and Aldo described 3 brothers with XP cutaneous manifestations and severe neurological degeneration start at 2 years of age and associated with dwarfism and immature sexual development .Gartler reported the presence of UV hpersensitivity of XP cells. DNA abnormalities in XP were first brought to attention of the general scientific community by the report of James cleaver in 1968 [3].
The incidence of XP is 1 in 250000 live births in United States [1]. Ethnicity was reported that the largest groups were from the Middle East, the 2nd frequency was in Europe, then Japan and the least in Africa [3]. Only 29 cases have been reported in Negroid (22 in Africa) [4].
XP is a rare hereditary disease characterized by hypersensitivity to sun rays. The clinical manifestations appear early in life, after the child is first exposed to sun light. Life expectancy is greatly reduced because of metastasis, infection or neurological complications [2]. From the study of 830 published cases, there is nearly an equal number of male and female [3]. The disease present with dry, thin skin with diffuse lentigo formation and usually present in early childhood. All forms of cutaneous malignancies may develop and death at young age from metastatic disease is almost inevitable [5]. The skin is normal at birth, the first symptoms are noticed between the 6th month and the 3rd year in most of the cases, but may appear in very early infancy or in later childhood .The rate of progression is unpredictable and has no constant relationship to the age at onset. Freckling and increasing dryness on light – exposed area are commonly the earliest symptoms. They vary in size from a very small to more than centimeter, vary in color from light to dark and may fuse to from larger patches of pigmentation. Small angiomata and telcangectases also appear in the course of the disease. Small, white atrophic spots are also added to the picture [6].
The manifestations of skin in XP can be highly reduced by protection from the damaging UV light. The patients must be aware to protect all body surfaces and especially the exposed surfaces from solar irradiation. When they go outdoors, the exposed skin surfaces must be protected by a topical sun screen (sun block) agents. Any agent or modality that minimizes the skin damage could greatly facilitate the patient care [2]. Enzymes such as T4 endonuclease V has shown some promise. Topical application of this enzyme increase the rate of repair of the sun light induced DNA damage in human cells [1].
Dermabrasion is a modality used in the treatment of XP which mechanically abrade the epidermis and the upper portion of the dermis to the depth sufficient to treat the disease [7]. Carbon dioxide laser recently provide an alternative option to treat the disease. The color of the skin is improved by mechanically removing the damaged skin, and the skin texture is improved by collagen shrinkage and remodeling [8]. Retinoids can be used and they act by affecting cell proliferation and differentiation. Studies have shown that retinoid can prevent the development of skin cancers especially in patient with XP. Affect the epidermis and the interface of the dermis-epidermis. Common agents used for superficial peel include: glycolic acid, 10-20% trichloro acetic acid, Jessener solution (recorcinol, salsylic acid and lactic acid), Unna paste (recorcinol, salsylic acid and zinc oxide), Tretinoin and Salicylic acid. Superficial peel cause mild erythema and desquamation and the healing time is about 4 days. Extend into the epidermis to the papillary dermis. Agents used for medium-depth peel are 35% trichloro acetic acid and phenol 88%. It causes erythema with moderate edema which heal in 5-7 days.
It penetrates the mid-reticular dermis. Agents used in deep peel include Baker solution and 50% trichloro acetic acid. The healing period is 2 weeks. The study was to evaluate the role of chemical peels in clearing the skin background in patients with XP and to decrease the rate of the development of new lesions.
Patients and Methods
Fourteen patients, 9 males and 5 females ranged in age from (1-30year) who were diagnosed to have XP by clinical examination were studied, evaluated and treated in the Burn and
Plastic surgery center in Al-Jamhuri Teaching Hospital in Mosul from March 2011 to May 2012.In all patients, a history was obtained with a physical examination of the skin and regional lymph nodes
.Ophthalmological examination of both eyes and ophthalmological consultation if needed. Routine investigation such as complete blood picture, ESR and other investigations were done when needed. Patient’s photographs were taken at first presentation, photographs also taken preoperatively and after one week, three weeks and six weeks post operatively during the period of the follow up after each session of chemical peeling.
The number of sessions depends on the severity of the disease and the assessment of the patient’s condition which was done by two plastic surgeons depending on several criteria including the number of
lesion, the degree of pigmentation and the decrease in freckling, scarring and wrinkles. Surgical excision was done for the skin lesions with different modalities for closure, including direct suturing, skin grafting and local skin flaps.
Chemical Peels:
Ten adult patients, underwent chemical peel, were treated with topical lidocain ointment while four child patients treated under general anesthesia.
The skin was degreased by alcohol. Trichloro acetic acid (TCA) in a concentration of (30%) was used for peeling the skin of the whole face. This concentration is prepared by adding water to (30gram) of Trichloro acetic acid crystal until 100 ml of solution is obtained (weight to volume) method. The solution was applied to the face with cotton tipped applicator. The solution was applied evenly and uniformly over the entire face in one pass (one touch) until frosting (white color) starts to appear which is usually about one minute after application of the acid.
At that time we applied an iced pack over the peeled areas with frequent change of the packs in order to relief pain associated with application of the acid. The procedure takes totally about 10 minutes. The patients were given local antibiotic ointment (fucidin) 3 times daily for 5 days and advised to avoid exposure to sun light and to use sun screen cream. Evaluation of the results was done by two plastic surgeons which are poor results in 2 cases, moderate in 7 cases and good results in 5 cases.
Results
Fourteen patients, 9 males and 5 females ranged in age from 1 year to 30 years. Three patients below 9 years, six patients aged between (10-19) years and five patients aged between (20-30) years. All of the patients were from areas and villages around and near the Mousl city. Eight patients are from Talaafar, three patients are from Makhmour, two patients are from Al-Mousl city, one patient is from Al-Hadhar. So we noted that the highest number is from Talaafar. One patient has no lesion; the other 13 patients develop collectively 70 lesions on which only 16 lesions were proved by the histopathologist as 9 basal cell carcinomas, 6 squamous cell carcinomas and 1 malignant melanoma.
We reported only 11 lesions treated by excision and split thickness skin graft, and 10 lesions closed by local flaps.
Three patients have neurological abnormalities as abnormal speech in three patients,
two patients are mentally retarded, one patient has deafness and one patient has ataxia. All of these 3 patients who have neurological abnormalities were from the same family.
Eleven patients have no neurological abnormalities. Ten patients have conjunctival congestion and 8 Patients have photophobia. The patients were submitted to chemical peeling in number of sessions.
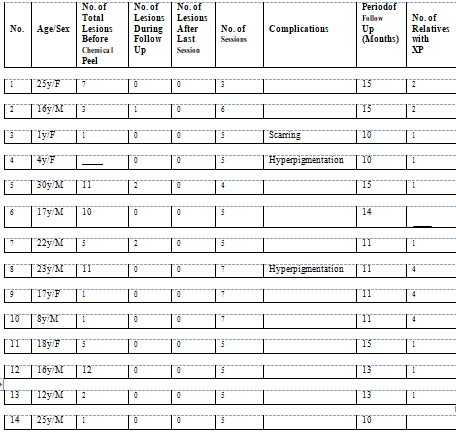
The interval between session and the other is about 3-4 weeks depending on the patient’s condition. One patient was undergone 3 sessions of chemical peeling, one patient was undergone 4 sessions of chemical peeling, eight patients were undergone 5 sessions of chemical peeling, one patient was undergone 6 sessions of chemical peeling and 3 patients were undergone 7 sessions of chemical peeling. No significant complications were developed as infection, hypo pigmentation and toxic shock syndrome, except scarring occurs in 1 case and hyper pigmentation occurs in 2 patients who can be ameliorated by early use of bleaching agent (Eldopaque 4%) and sun screen. The duration of the period of the follow up of the patients ranged from a minimum of 10 months to 15 months. During this period 3 patients develop lesions,
2 of them develop 2 lesions and 1 of them develops 1 lesion after the starting of the chemical peeling. All these lesions were benign which were proved by FNAC and showed no evidence of malignant cells (table1).
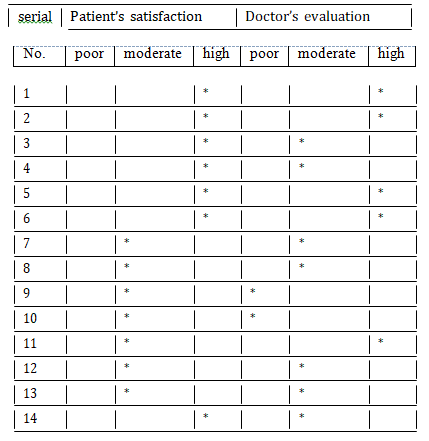
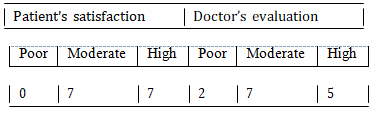
Two of these lesions was excised surgically and 3 of them were removed by chemical peeling and they disappear completely. The aesthetic results were evaluated by either patient satisfaction which was classified into 3 degrees which depend on the patient himself or his parent as unsatisfied, moderately satisfied but seek more or highly satisfied. We found that seven patients were highly satisfied and seven patients were moderately satisfied (table3). The other indicator for the aesthetic result is doctor’s evaluation in which we consult two plastic surgeons by showing them two pictures of each patient, preoperatively and postoperatively and allowing to decide the result wither poor (no changes occur), fair (improvement in skin background, decreases in freckling, wrinkles, pigmentation, and fine scars) and good aesthetic results (further and more improvement in skin background) (table 1).
Table 1. Details of the Patients
Table 2. showing the degree of patient’s satisfaction and doctor’s evaluation.
Table 3. showing the summary of patient’s satisfaction and doctor’s evaluation.
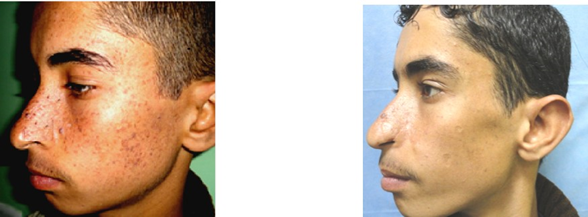
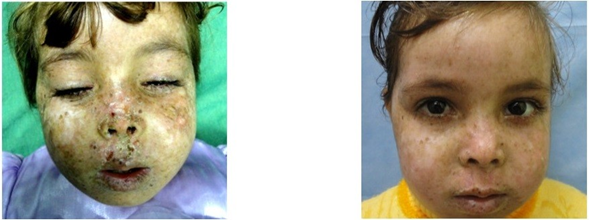
Figure 1. Patient No.1: 16 year
Figure 2. Patient No2: 4 years
Discussion
In this study, the highest incidence of XP is in the age of 10-29 year old which may be due to the fact that most of them usually reach the age of malignancy at this age period, so they consult the plastic surgeon, this goes with the data written in the text book of dermatology [6]. In our small sample of patients, the disease is predominant in male. It does not go with the study done by Kreamer and Myung on 830 cases from all over the world with nearly equal number of male and female [3] .this attributed to that males in Iraq are more sun exposed and could attend hospitals more than females. Thirteen patients in this study have positive family history in the same family and in first and second cousins, one patient is with negative family history .This mean that the disease goes in families and is related to consanguineous marriage [9] which is a common habit in our community. The skin is degreased by alcohol which is advocated by many authors to removes excess oil and facilitates the penetration of the peeling agent [10]. The concentration of 30% tri chloro acetic acid solution is prepared by using (weight to volume) method. This method is advocated by many authors as it gives a uniform and comparable study and is better than other methods of tri chloro acetic acid preparation [11].
The number of the sessions of chemical peels who have been done in those 14 patients ranged from 3 sessions to 7 sessions. It depend on the severity of the disease and the response and the improvement of the patients .The number of sessions in this study goes with the study done by Wee Seong who perform chemical peeling using 40% tri chloro acetic acid 5 times for his patient and notice an improvement of the patient[2]. The peeling procedure was well tolerated by most of our patients, there is no bleeding, no pain intra operatively and post operatively [5].
Some of the patients were treated with topical lidocain ointment which provides a comfortable state for both the patients and
the surgeon. This goes with the Huang et al study who noted that local anesthesia is frequently preferred by the plastic surgeons because of its effectiveness in permitting patient
cooperation during the operation [12]. Other patients (children) were treated under general anesthesia using ketamin agent in a single induction dose
which has the advantages of being hypnotic, strong analgesic and short duration of action and allows rapid recovery from anesthesia with post-operative analgesia.
Fortunately, no significant complications occur following chemical peeling. The hyper pigmentation that occur perhaps due to tendency of the patients with XP for
hyper pigmentation which is caused by exposure to sun light and because they did not follow the preventive measures [13].
The scarring may be due to deep peeling with delay in application of iced packs which prevent deep penetration of the acid .No infection were reported which is due to
well preparation of the patients before the procedure with the use of local antibiotic to the peeled areas post operatively. An important subject to discuss is the development of new lesions after chemical peels. We notice that the patients in this study have a less tendency to develop lesions after they have been undergone chemical peeling which reflects the potential of some prevention of new lesions development which might change to malignancy.
This goes with the studies which have been assumed that chemical peels have provide a prophylactic effect against the development of skin malignancies in which they eliminate all subclinical premalignant lesions and it can clear obscuring background skin changes [5,13]. Also this goes with the studies that have been assumed that chemical peels have the same effect of dermabrasion in the prevention of the development of skin lesions [5,13]. Regarding the aesthetic purpose, the technique increase self-esteem and improve quality of life because it substitute the dry, hyper pigmented and atrophied skin by a smooth, nice and lesion free skin and the patient not only benefit from removal of the erythromatous, scaly actinic keratoses but also obtain cosmetically pleasing rejuvenation of facial skin and diminution of fine facial wrinkles [5,13].
Those patients who were undergone chemical peels notice the development of new lesions easily so they consult their doctors for treatment earlier than those with full face lesions who cannot easily notice the development of new lesions [10].The improvement of their facial appearance will become a stimulating factor for those patients to take a more preventive measures such as avoiding sun exposure by cover the exposed body surfaces, not going out doors and the use of sun block creams. I think that the drawbacks of this study are the small number of patients treated by this method and the relatively short period of the follow up of the patients.
Conclusion & Recomendations
From our study, it is evident that chemical peels offer a simple and well-tolerated procedure for patients, accompanied by minimal discomfort and negligible side effects. The treatment has demonstrated satisfactory results, effectively reducing freckles and pigmentations on patients’ faces while keeping complications to a minimum.
To ensure the well-being of patients with XP and enhance the effectiveness of their treatment, we recommend the following measures:
Preventive Measures: Patients should take proactive steps to minimize sun exposure. This includes refraining from outdoor activities during peak sunlight hours, protecting
all exposed body surfaces, and consistently applying high-quality sunblock creams. These precautions are crucial to reduce the risk of skin damage and potential complications.
Regular Skin Examinations: Patients, their parents, or healthcare providers should conduct regular skin
examinations. This practice helps in the early detection of new lesions and any changes in the skin, enabling prompt intervention when necessary.
Early Intervention with Chemical Peels: Consider chemical peels as an early treatment option when
there is suspicion of new lesion development. This approach can effectively target subclinical lesions, potentially delaying or preventing the emergence of new tumors. Early intervention is vital for the effective management of XP.
Future Research: We recommend conducting future studies with a larger number of patients and
extending the duration of the follow-up period. Comparing the results of chemical peel treatments with other modalities for XP management would provide
valuable insights into the most effective approaches for treating this condition.
Further research can contribute to improved patient care and outcomes in the long term. This would enhance our understanding of XP treatment options and the overall well-being of affected individuals.
Acknowledgments: The authors would like to appreciate patients who agree to participate and follow the study protocol patiently
Author Contributions: All authors contributed equally to the writing of this paper. All authors read and approved
the final manuscript.
Conflicts of Interest: The authors declare that they do not have any conflict of interests.
References
Barton M.R. "Malignant tumor of the skin" in: Mathes J.S. and Hentz R.V. eds. Plastic surgery: "Tumors of the head, neck and skin" ,2nd ed., Philadelphia ,2006, vol.5 ,297_280.
Wee, Seong Yun, and Duck-Sun Ahn. "Facial resurfacing in xeroderma pigmentosum with chemical peeling." Plastic and reconstructive surgery 103.5 (1999): 1464-1467. https://journals.lww.com/plasreconsurg/citation/1999/04020/facial_resurfacing_in_xeroderma_pigmentosum_with.16.aspx
Kraemer, Kenneth H., Myung M. Lee, and Joseph Scotto. "Xeroderma pigmentosum: cutaneous, ocular, and neurologic abnormalities in 830 published cases." Archives of dermatology 123.2 (1987): 241-250.https://jamanetwork.com/journals/jamadermatology/article-abstract/548003
Herbert. U.C. Lefate, J.F., Herbert.O., Xeroderma pigmentosum in nergroid childern in "AnnDermatolVenereol" 1994,121(5):382
Akan, I. M., et al. "Combined treatment of xeroderma pigmentosum with full-face chemical peeling and dermabrasion." European Journal of Plastic Surgery 24 (2001): 243-246.DOI: https://doi.org/10.1007/s002380100282
Burton J.L and Rook A." Gentics in dermatology" in Burns T., Breathnach S., Cox N .and Griffths C. ed.
"Rooks text book of dermatology", 8th ed.,Wiley-BlackWell, 2010, vol.146-147.
Perotti A. J. ,Cutaneous resurfacing : Chemical peeling ,Dermabrasion and Laser resurfacing in: Thorne H.C. ed. ,Grabb and Smith Plastic Surgery 6th , Lippincott Williams and wilkins , 2007 ,vol. 1, 112.
Grossman, Melanie C., A. N. Kauvar, and R. G. Geronemus. "Cutaneous laser surgery." Grabb and Smith’s Plastic Surgery. 5th ed. Philadelphia: Lippincott-Raven (1997).
Beloti J., Coulter D. DNA: Its mutation ,repair and recombination in :Tamarin H.R. Ed. "Princeples of genitics" ,7th ed. ,
New York ,John Wiley and Sons ,1984 , chap 9, 316.
Nelson, Bruce R., et al. "The role of dermabrasion and chemical peels in the treatment of patients with xeroderma pigmentosum." Journal of the American Academy of Dermatology 32.4 (1995): 623-626.https://doi.org/10.1016/0190-9622(95)90348-8
Vossen, Marieke, J. Joris Hage, and Refaat B. Karim. "Formulation of trichloroacetic acid peeling solution: a bibliometric analysis." Plastic and reconstructive surgery 105.3 (2000): 1088-1094.https://journals.lww.com/plasreconsurg/abstract/2000/03000/formulation_of_trichloroacetic_acid_peeling.38.aspx
Del Pizzo, A., and A. Tanski. "Chemical face peeling--malignant therapy for benign disease?." Plastic and Reconstructive Surgery 66.1 (1980): 121-123.https://europepmc.org/article/med/7394032
damage of the face and scalp . J. Am. Acad. Dermatol. 1996. 34(4) :638_44.
Advertisement
Recommended Articles
Research Article
abc
Published: 30/06/2024
Download PDF
Cite
x
APA
(2024). abc. Himalayan Journal of Medicine and Surgery, 5(1), 2-10.
MLA
. "abc." Himalayan Journal of Medicine and Surgery 5.1 (2024): 2-10.
Chicago
. "abc." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 2-10.
Harvard
(2024) 'abc' Himalayan Journal of Medicine and Surgery 5(1), pp. 2-10.
Vancouver
. abc. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):2-10.
Download PDF
Research Article
Transformative Applications in Genetic Disorders and Cancer Therapy, Ethical Considerations, and Future Prospects
Kritika Dod,
Esha Singh
Published: 30/06/2024
Download PDF
Cite
x
APA
Dod, K. & Singh, E. (2024). Transformative Applications in Genetic Disorders and Cancer Therapy, Ethical Considerations, and Future Prospects. Himalayan Journal of Medicine and Surgery, 5(1), 1-4.
MLA
Dod, Kritika and Esha Singh. "Transformative Applications in Genetic Disorders and Cancer Therapy, Ethical Considerations, and Future Prospects." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-4.
Chicago
Dod, Kritika and Esha Singh. "Transformative Applications in Genetic Disorders and Cancer Therapy, Ethical Considerations, and Future Prospects." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-4.
Harvard
Dod, K. and Singh, E. (2024) 'Transformative Applications in Genetic Disorders and Cancer Therapy, Ethical Considerations, and Future Prospects' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-4.
Vancouver
Dod K, Singh E. Transformative Applications in Genetic Disorders and Cancer Therapy, Ethical Considerations, and Future Prospects. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-4.
Download PDF
Research Article
Stroke Knowledge in Shimla: Identifying Symptoms and Prevention Tactics
Lavinder Kumar
Published: 20/05/2024
Download PDF
Cite
x
APA
Kumar, L. (2024). Stroke Knowledge in Shimla: Identifying Symptoms and Prevention Tactics. Himalayan Journal of Medicine and Surgery, 5(1), 1-8.
MLA
Kumar, Lavinder. "Stroke Knowledge in Shimla: Identifying Symptoms and Prevention Tactics." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-8.
Chicago
Kumar, Lavinder. "Stroke Knowledge in Shimla: Identifying Symptoms and Prevention Tactics." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-8.
Harvard
Kumar, L. (2024) 'Stroke Knowledge in Shimla: Identifying Symptoms and Prevention Tactics' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-8.
Vancouver
Kumar L. Stroke Knowledge in Shimla: Identifying Symptoms and Prevention Tactics. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-8.
Download PDF
Research Article
Understanding Hemorrhoids: Assessing Awareness and Knowledge in Bilaspur
Kartik guleria,
...
Prashant Sharma
Published: 20/06/2024
Download PDF
Cite
x
APA
guleria, K., kanwar, S. & Sharma, P. (2024). Understanding Hemorrhoids: Assessing Awareness and Knowledge in Bilaspur. Himalayan Journal of Medicine and Surgery, 5(1), 1-7.
MLA
guleria, Kartik, Shipra kanwar and Prashant Sharma. "Understanding Hemorrhoids: Assessing Awareness and Knowledge in Bilaspur." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-7.
Chicago
guleria, Kartik, Shipra kanwar and Prashant Sharma. "Understanding Hemorrhoids: Assessing Awareness and Knowledge in Bilaspur." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-7.
Harvard
guleria, K., kanwar, S. and Sharma, P. (2024) 'Understanding Hemorrhoids: Assessing Awareness and Knowledge in Bilaspur' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-7.
Vancouver
guleria K, kanwar S, Sharma P. Understanding Hemorrhoids: Assessing Awareness and Knowledge in Bilaspur. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-7.
Abdulrazaq*, B. H., Sadoon, H. H. & Abdulrazaq, G. A. (2023). Evaluation of the Role of Chemical Peel in the Treatment of Xeroderma Pigmentosum. Himalayan Journal of Medicine and Surgery, 4(2), 1-7.
MLA
Abdulrazaq*, Basil H., Haider H. Sadoon and Ghassan A. Abdulrazaq. "Evaluation of the Role of Chemical Peel in the Treatment of Xeroderma Pigmentosum." Himalayan Journal of Medicine and Surgery 4.2 (2023): 1-7.
Chicago
Abdulrazaq*, Basil H., Haider H. Sadoon and Ghassan A. Abdulrazaq. "Evaluation of the Role of Chemical Peel in the Treatment of Xeroderma Pigmentosum." Himalayan Journal of Medicine and Surgery 4, no. 2 (2023): 1-7.
Harvard
Abdulrazaq*, B. H., Sadoon, H. H. and Abdulrazaq, G. A. (2023) 'Evaluation of the Role of Chemical Peel in the Treatment of Xeroderma Pigmentosum' Himalayan Journal of Medicine and Surgery 4(2), pp. 1-7.
Vancouver
Abdulrazaq* BH, Sadoon HH, Abdulrazaq GA. Evaluation of the Role of Chemical Peel in the Treatment of Xeroderma Pigmentosum. Himalayan Journal of Medicine and Surgery. 2023 Jul;4(2):1-7.