The ongoing global problem of concern is the Coronavirus Disease 2019 (COVID-19) caused by the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). With the sudden explosion of the disease, no drugs were experimentally proven in its management. This meta-analysis assessed the role of favipiravir in the management of COVID 19 disease, its efficacy and safety. A comprehensive search of databases including PubMed, Medline, Cochrane, Embase, Google scholar, Lancet, Elsevier and other modalities of search like website searching and citation tracking was made. Out of 687 articles identified, 8 articles were taken for the meta-analysis after several stages of exclusion. Out of the 8 studies selected, the results of 4 studies were in favor of favipiravir, while other 4 studies were against the efficacy of favipiravir. The result of our statistical analysis was that RR = 0.9276 (95% CI; 0.6718 to 1.3944) for the effect of favipiravir on mortality reduction in COVID 19 patients. Favipiravir treatment in the early phase of infection (viral replication phase) have shown significant reduction in the viral load and good clinical recovery. It also prevents the progression of disease to critical stage by controlling the infection adequately in the early phase itself. But when the stage of viral replication has passed, there is no role of favipiravir in the management of the COVID 19 disease. Favipiravir has no significant effect on mortality reduction in COVID 19 patients.
Keywords
Antivirals
COVID 19
Favipiravir
Pharmacotherapy
Repurposing Drugs
SARS CoV 2
INTRODUCTION
The ongoing global problem of concern is the Coronavirus Disease 2019 (COVID-19) caused by the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). COVID-19 disease manifests grossly in 2 phases: The early phase of mild illness is caused by the virus followed by a late phase of severe and critical illness which is solely constituted by dysregulated inflammatory and immune responses [1]. It is crucial to understand the course of the disease while aiming for treatment, as the treatment modality varies with the various stages. Early intervention, when possible, should predominantly target the viral multiplication that can largely limit the progression of the disease and the aftermath [2].
With the compelling need to discover therapeutic options for COVID-19 disease, the idea of repurposing the existing drugs were thought [3]. Favipiravir, a purine nucleic acid analogue was initially developed by Toyama Chemical Co., Ltd. in Japan for the treatment of mild viral infections.[4] It acts by inhibiting RNA Dependent RNA Polymerase enzyme (RDRP), thereby hindering the multiplication of RNA viruses [5]. Ever since the COVID-19 disease was reported a pandemic, the role of favipiravir against SARS-CoV-2 was being evaluated. Various studies on favipiravir conducted during this crisis have shown mixed results: some regard it as a promising choice while others regard it as not of much significance. The intent of this meta-analysis is to assess the role of favipiravir, it’s safety and efficacy in the treatment of COVID-19.
MATERIALS AND METHODS
This systematic review was performed in strict accordance with the Preferred Reporting Items of the Systematic review and Meta-Analysis (PRISMA) checklist. All steps were compliant with the Cochrane Handbook of Systematic Review and Meta-Analysis.
Search Strategy
We conducted a comprehensive literature review by searching the databases like PubMed, Medline, Cochrane, Embase, Google scholar, Lancet, Elsevier. The following search terms were used: ‘Favipiravir’ ‘Drug trials’ ‘Pharmacotherapy’ ‘randomized control trials’ ‘antivirals. The search also included mining references from good quality articles, website searching and citation tracking.
Inclusion Criteria
Studies on COVID-19 conducted between April 2020 and July 2021
Studies on pharmacotherapy for COVID-19 specially focusing favipiravir
Studies with sample size >100
Studies with good methodologies
Studies with properly outlined efficacy and safety endpoints of favipiravir
Exclusion Criteria
Articles on COVID published before 2020
Studies showing in-vitro effects of favipiravir
Abstract-only papers, articles with full texts not available
Articles with only guidelines/protocol for management of COVID 19
Articles published in languages other than English
Data Extraction
The data was extracted independently from the eligible studies. The reliability of the data was cross-checked by reviewing the same article in multiple other systematic reviews of various authors. Generic inverse variance method (random-effects model) was used to estimate the Odds Ratios (OR) of patients for primary outcome variables with 95% Confidence Intervals (CI). Results after adjustments and propensity score matching were taken to eliminate ‘Selection bias’.
Statistical Analysis
The odds ratios with 95% confidence intervals of the individual studies were compiled. The data were processed using the Statistical Package for the Social Sciences (SPSS) software version 20.0.
RESULTS
Study Selection
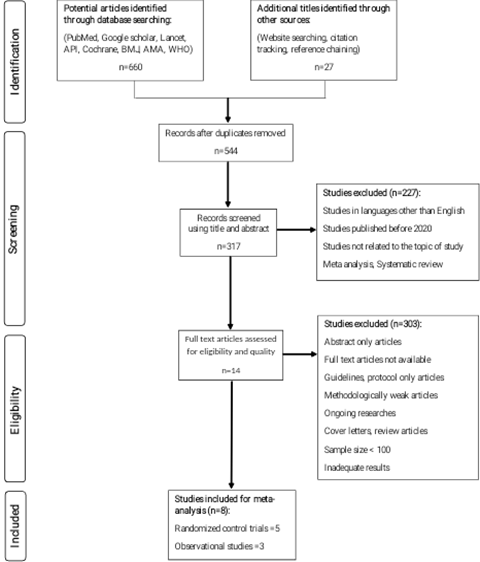
A total of 687 articles were identified via database searches, website searching and reference chaining. After eliminating duplicate studies (143), articles that were inappropriate to the study topic (227) and articles that did not fit the eligibility criteria (303), 14 articles were eligible. After quality assessment, 8 articles were taken for the meta-analysis, of which 5 were Randomized control trials and 3 were Observational studies (Figure 1).
Study Characteristics
The studies were chosen based on the following details: date of publication, study design, country where the study was conducted, sample size, number of patients in the intervention group - treated with favipiravir, combination of drugs if given, number of deaths, number of ICU admissions, invasive mechanical ventilation, viral clearance time, length of hospital stay, comorbidities and number of patients in the control group who received standard care of treatment/placebo.
Synthesis of Results
In our meta-analysis, the following parameters wereevaluated:
Time taken for clinical recovery
Length of hospital stay
Changes in SpO2 levels during hospitalization
Mortality
Data of 4304 patients collected from 8 studies conducted in different parts of the world are shown in Table 1.
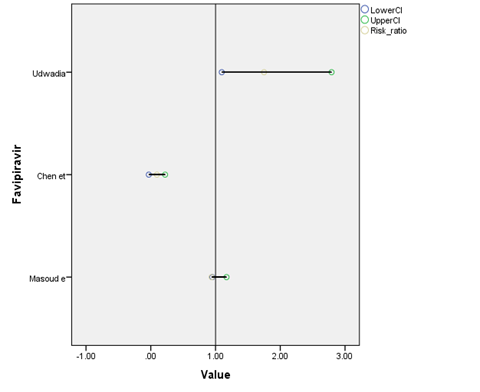
Out of the 8 studies selected, the results of 4 studies were in favour of the use of favipiravir, while other 4 studies were against the efficacy of favipiravir. The result of our statistical analysis was that the relative risk (Figure 2) for mortality reduction of favipiravir in COVID 19 patients is 0.9276 (95% CI; 0.6718 to 1.3944).
Risk of Bias Assessment
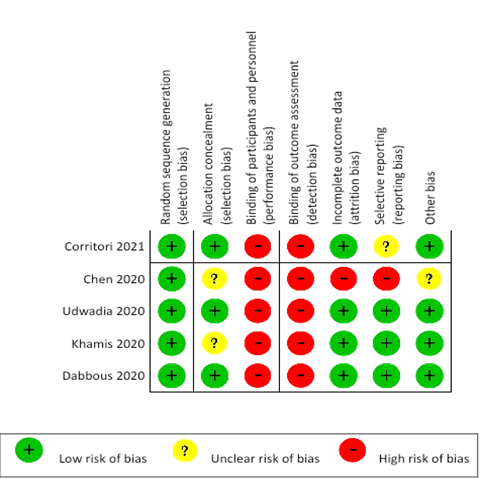
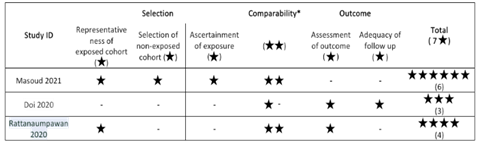
We assessed the risk of bias (‘low risk’, ‘unclear’, or ‘high risk’) for the studies included in the meta-analysis using version 2 of the Cochrane Risk of Bias assessment tool for randomized control trials (Figure 3) and The New Castle Ottawa scale for non-randomized controlled trials (Table 2). Disagreements aroused during this process were resolved through discussion. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was utilized to assess the quality of the evidence obtained from various studies.
DISCUSSION
SARS CoV-2 is a single stranded positive sense RNA virus belonging to the corona viridae family. It is an enveloped virus with spike proteins on its surface [14]. The virus encodes proteases and the enzyme RNA-dependent RNA polymerase (RdRp) [15]. Both RdRp and viral proteases were considered as prime targets for the development of potential therapeutic agents. Favipiravir is one such attempt.
Previously known as T-705, favipiravir (6-fluoro-3-hydroxypyrazine-2-carboxamid) is a pro-drug. Intracellularly, it undergoes ribosylation and phosphorylation to form favipiravir ribofuranosyl-5′-triphosphate (Favipiravir- RTP), the active metabolite. Favipiravir-RTP competes with purine nucleosides and hinders the viral replication. It integrates with the nascent viral RNA causing inhibition of viral RdRp which leads to termination of the chain and viral mutations [16]. Oral favipiravir is well absorbed with bioavailability of nearly 97.6%. Like most of the drugs, favipiravir is metabolized in liver, mostly by Aldehyde Oxidase enzyme and partly it is converted to a hydroxylated form by the enzyme Xanthine Oxidase. The hydroxylated form is then excreted by the kidneys [17,18].
Time Taken for Clinical Recovery
In an observational study of 380 patients conducted by Masoud et al. in Iran, treatment with favipiravir showed no difference in the time taken for clinical recovery when compared to the control group. The hazard ratio calculated using Cox proportional hazard modelling was 0.94 (95% CI: 0.75-1.17) [6]. The results were similar to that of the RCT conducted by Chang Chen et al. in China with 240 patients.
Figure 1: Prisma Flow Chart Showing Study Selection
Figure 2: Relative Risk of Mortality Reduction of Favipiravir as Per the Analyzed Studies
The difference of recovery rate was 0.0954 (95% CI: 0.0305-0.2213) between the favipiravir group and the arbidol (control) group.[10] Further studies by Yohei Doi et al. in Japan involving 2158 patients [7] and by Pinyo Rattanaumpawan et al. in Thailand involving 247 patients [9] also showed results that were consistent that time taken for clinical recovery in patients taking favipiravir and that of the control group was almost alike.
Length Of Stay in Hospital
When observed the medically discharged patients as per physician’s advice in Masoud et al. study [6], the median length of hospital stay was 7 days in the favipiravir group and 6 days in the control group (p = 0.85).
Figure 3: The Cochrane Risk of Bias Assessment for Randomized Control Trial Studies Analyzed
There was no significant variation between the results of the two groups. This is supported by the Randomized controlled trial conducted on 89 patients by Faryal Khamis et al. at Oman [12]. The length of stay in hospital was similar in the favipiravir and the control group (p = 0.948).
Spo2 Change Over-Hospitalization
In the observational study by Masoud et al. [6], out of 380 patients taken in the study, 193 patients were on favipiravir and 187 were on lopinavir/ ritonavir. Supplemental oxygen was paused for 5 minutes in un-intubated patients among the two groups to look for changes in the oxygen saturation (SpO2). The results were indistinguishable (OR = 1.00, 95% CI: 0.71–1.42; p = 0.997).
Mortality
In the Randomised controlled trial on 89 patients conducted by Faryal Khamis et al. in Oman [12], the mortality rates were 11.4% and 13.3% in the favipiravir and the non-favipiravir group (p = 0.778). The results did not significantly differ among the two groups. It is in accordance to the results of Masoud et al. study [6], where the number of deaths were 26 in the favipiravir group and 21 in the Lopinavir/Ritonavir group among the 47 deaths (p = 0.49).
The possible explanation that could be regarded for the negative findings on the efficacy of Favipiravir against COVID 19 disease could be explained by the pathogenesis of this disease. The disease course includes 2 phases: The early phase of infection usually occurs in first 1 week from the day of acquiring the virus. Patients experience mild symptoms or are mostly asymptomatic. [19,20] When infection not controlled in the early phase due to factors like immunosuppressed state, immunocompromised patients, patients with comorbidities like diabetes, coronary artery disease, the patients progress to the later stage of the disease, which is constituted by a surge of inflammatory reactions in response to the uncontrolled viral load.
Table 1: Summary of studies analyzed in the meta-analysis
Study ID
Country
Study Design
Sample Size
Experimental Group
Comparative Group
Results
Description
Masoud et al.
[6]
Iran
Multicenter observational study
380
Patients treated with favipiravir (193)
Patients treated with lopinavir/ ritonavir (187)
HR = 0.94 for clinical recovery in patients taking favipiravir vs lopinavir/ ritonavir.
Hospital stays and the time to clinical recovery of patients with favipiravir did not vary when compared to lopinavir and ritonavir.
Yohei Doi et al. (2020) [7]
Japan
Observational study
2158
-
-
Rates of symptomatic improvement were 87.8%, 84.5% and 60.3% at 14 days for mild, moderate and severe disease, respectively.
Majority of patients who had taken favipiravir have had significant improvement and recovery of illness.
Corritori et al. [8]
Russia
RCT
940
Patients who took favipiravir (470)
Patients on standard care (470)
Median time of viral clearance in favipiravir group and standard care are 6 and 12 days, respectively.
Favipiravir has a high clinical efficacy and tolerability in covid 19 patients.
Pinyo Rattanaumpawan et al. [9]
Thailand
Multicentre observational study
247
Patients who received Favipiravir (63)
Patients who did not receive Favipiravir (184)
The clinical improvement rate on day 7 was 66.7% in all patients, 92.5% in patients who did not require O2-supplementation and 47.2% in patients who required O2-supplementation.
Favipiravir shows promising effects in Covid-19.
Chang Chen et al. [10]
China
Prospective, open-label multicenter RCT
240
Patients who received Favipiravir (120)
Patients who received arbidol (120)
On day 7, the clinical recovery rate did not significantly vary between Favipiravir group (71/116) and Arbidol group (62/120).
Favipiravir did not significantly improve clinical recovery rate when compared with arbidol.
Zarir F. Udwadia et al. [11]
India
Open-label, parallel-arm, multicenter RCT
150
Patients treated with favipiravir (75)
Patients not treated with favipiravir (75)
Median time to clinical improvement of symptoms was 3 days in the favipiravir group vs 5 days in the control group.
In mild to moderate COVID 19 patients, use of favipiravir showed significant clinical improvement in 3 days.
Faryal Khamis et al. [12]
Oman
Open-label RCT
89
Patients who received Favipiravir + inhaled interferon beta-1b (44)
Patients who received HCQ (45)
The mortality rates were 11.4% and 13.3% in patients who received Favipiravir + inhaled interferon beta-1b and HCQ, respectively.
There was no significant reduction in mortality among hospitalised patients who received Favipiravir and inhaled interferon beta-1b combination therapy.
Hany M. Dabbous et al. [13]
Egypt
RCT
100
Patients treated with favipiravir (50)
Patients treated with HCQ + Oseltamivir (50)
PCR seronegative conversion on day 7 was 48% and 55.1% in the favipiravir and HCQ + oseltamivir groups, respectively.
In mild to moderate COVID 19 patients, treatment with favipiravir showed similar effects to that of HCQ and oseltamivir combination therapy.
This gush of immune and inflammatory mediators is called the ‘cytokine shower’ and when it is massive, it is called the ‘cytokine storm’ [21-23]. Therefore, treatment in the early phase should aim the viral replication and in late phase should target the cytokine storm. If the patients included in the above studies had passed the viral replication phase, they are unlikely to benefit from the antiviral treatment.
Adverse Events
Favipiravir is a drug with well-established safety profile and is usually tolerated well. The frequently reported adverse effects were diarrhea, increased serum uric acid level, reduction of neutrophil count and abnormal liver function tests showing raised transaminases (AST, ALT) [24]. On further evaluation of patients who had increased serum uric acid level, it was found that they had developed Acute Kidney Injury (AKI). They were non-oliguric; urine analysis was unremarkable and ultrasound showed features of neither obstructive uropathy nor renal vasculature thrombosis. The AKI improved within 24-48 hours of discontinuation of favipiravir treatment, eliciting the association with the drug. The respiratory failure of the patients had resolved and inflammatory markers were lowered which eliminates the possibility of direct SARS-CoV-2 related AKI. This suggests that the AKI caused was ‘drug induced nephrotoxicity’ [25].
Favipiravir causing teratogenicity and early embryonic lethality have been observed in several animal models. Therefore, premenopausal women should be cautioned and pregnancy must be excluded before initiating favipiravir treatment. It is also essential that all patients and their sexual partners practice safe contraception during the treatment course and till 10 days after the end of favipiravir therapy [26].
Table 2: The New Castle Ottawa Scale for Non-Randomized Controlled Trial Studies Analyzed
Limitations
Our study had two limitations. One, not all studies were Randomised controlled trials, which increases the risk of bias. Two, only 8 studies were taken for the review as no other studies were qualitatively and quantitatively eligible to take up. Many randomized controlled trials with ample sample size, reliable data collection and good quality results are necessary to arrive at more beneficial outcomes.
CONCLUSION
Favipiravir treatment in the early phase of infection (viral replication phase) have shown significant reduction in the viral load and good clinical recovery. It also prevents the progression of disease to critical stage by controlling the infection adequately in the early phase itself. But when the stage of viral replication has passed, there is no role of favipiravir in the management of the COVID 19 disease. Favipiravir has no significant effect on mortality reduction in COVID 19 patients.
Acknowledgment
We thank Ms. Sumithra. Department of Statistics from Manonmaniam Sundaranar University, Tirunelveli for helping us with the statistical analysis of our results. We also thank David Sam Selva Jeyam, medical scholar from Tirunelveli Medical College for helping us with the technical aspects of the write up.
REFERENCES
S. Srikumar and S. Perumal. "A systematic review of immune pathogenesis of sars-cov-2 infection." International Journal of Advanced Medicine, vol. 8, 2021, pp. 978–983.
Y. Furuta et al. "Favipiravir (T-705), a broad-spectrum inhibitor of viral rna polymerase." Proceedings of the Japan Academy, Series B, Physical and Biological Sciences, vol. 93, no. 7, 2017, pp. 449–463. https://doi.org/10.2183/pjab.93.027.
J. S. Lee et al. "Anti-Ebola therapy for patients with ebola virus disease: a systematic review." BMC Infectious Diseases, vol. 19, no. 1, 2019, p. 376. https://doi.org/10.1186/s12879-019-3980-9.
FUJIFILM Toyama Chemical Co., Ltd. Drug Interview Form: Avigan®. http://fftc.fujifilm.co.jp/med/abigan/pack/pdf/abigan_if_01.pdf. Accessed 5 Apr. 2020.
T. Manabe et al. "Favipiravir for the treatment of patients with covid-19: a systematic review and meta-analysis." BMC Infectious Diseases, vol. 21, no. 1, 2021, p. 489. https://doi.org/10.1186/s12879-021-06164-x.
M. Solaymani-Dodaran et al. "Safety and Efficacy of Favipiravir in Moderate to Severe SARS-CoV-2 Pneumonia." International Immunopharmacology, vol. 95, 2021, p. 107522. https://doi.org/10.1016/j.intimp.2021.107522.
Doi, Yohei et al. Preliminary Report of the Favipiravir Observational Study in Japan. 15 May 2020. https://doi.org/10.1101/2020.05.15.20100334.
S. Corritori et al. "Favipiravir clinical outcomes." Topics in Antiviral Medicine, vol. 29, no. 1, 2021, p. 138.
Rattanaumpawan, Pinyo et al. Favipiravir in COVID-19: Clinical Outcomes. medRxiv, 2020. https://doi.org/10.1101/2020.06.24.20133249.
C. Chen et al. "Favipiravir versus arbidol for clinical recovery rate in moderate and severe adult COVID-19 patients: A prospective, multicenter, open-label, randomized controlled clinical trial." Frontiers in Pharmacology, vol. 12, 2021, p. 683296. https://doi.org/10.3389/fphar.2021.683296.
Z. F. Udwadia et al. "Efficacy and safety of favipiravir, an oral rna-dependent rna polymerase inhibitor, in mild-to-moderate covid-19: a randomized, comparative, Open-Label, Multicenter, Phase 3 Clinical Trial." International Journal of Infectious Diseases, vol. 103, 2021, pp. 62–71. https://doi.org/10.1016/j.ijid.2020.11.142.
F. Khamis et al. "Randomized Controlled Open Label Trial on the Use of Favipiravir Combined with Inhaled Interferon Beta-1b in Hospitalized Patients with Moderate to Severe COVID-19 Pneumonia." International Journal of Infectious Diseases, vol. 102, 2021, pp. 538–543. https://doi.org/10.1016/j.ijid.2020.11.008.
H.M. Dabbous et al. "Safety and Efficacy of Favipiravir Versus Hydroxychloroquine in Management of COVID-19: A Randomised Controlled Trial." Scientific Reports, vol. 11, no. 1, 2021, p. 7282. https://doi.org/10.1038/s41598-021-85227-0. [Retracted].
A. Zumla et al. "Coronaviruses—Drug Discovery and Therapeutic Options." Nature Reviews Drug Discovery, vol. 15, no. 5, 2016, pp. 327–347.
A. Vora and M. Tiwaskar. "Favipiravir." Journal of the Association of Physicians of India, vol. 68, no. 8, 2020, pp. 91–92.
A. Shannon et al. bioRxiv, 1 Jan. 2020. https://doi.org/10.1101/2020.02.08.939751.
Y.X. Du et al. "Clinical Pharmacology Consideration on Favipiravir Use in COVID-19." Clinical Pharmacology & Therapeutics, 30 Apr. 2020. https://doi.org/10.1002/cpt.1878.
Avigan [Package Insert]. Toyama Chemical Co. Ltd., Japan, 2017.
M. Catanzaro et al. "Immune Response in COVID-19: Addressing a Pharmacological Challenge by Targeting Pathways Triggered by SARS-CoV-2." Signal Transduction and Targeted Therapy, vol. 5, no. 1, 2020, p. 84. https://doi.org/10.1038/s41392-020-0191-1.
H.K. Siddiqi and M.R. Mehra. "COVID-19 Illness in Native and Immunosuppressed States: A Clinical-Therapeutic Staging Proposal." Journal of Heart and Lung Transplantation, vol. 39, no. 5, 2020, pp. 405–407. https://doi.org/10.1016/j.healun.2020.03.012.
J. Wu, W. Li and X. Shi. "Early Antiviral Treatment Contributes to Alleviate the Severity and Improve the Prognosis of Patients with Novel Coronavirus Disease (COVID-19)." Journal of Internal Medicine, vol. 288, no. 1, 2020, pp. 128–138. https://doi.org/10.1111/joim.13063.
R. J. Mason "Pathogenesis of COVID-19 from a cell biology perspective." European Respiratory Journal, vol. 55, no. 4, 2020, p. 2000607. https://doi.org/10.1183/13993003.00607-2020.
D. Giammaria and A. Pajewski. "Can Early Treatment of Patients with Risk Factors Contribute to Managing the COVID-19 Pandemic?" Journal of Global Health, vol. 10, no. 1, 2020. https://doi.org/10.7189/jogh.10.010377.
Fabiflu. Glenmark Pharmaceuticals Ltd., Mumbai, India, 2020.
Nasa, Prashant et al.
“Pharmaceuticals and Medical Devices Agency”. Report on the Deliberation Results of Avigan Tablet 200 mg. 2014, https://www.pmda.go.jp/files/000210319.pdf.
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Medicine and Surgery open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Advertisement
Recommended Articles
Research Article
Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori
Noor Zuhair Bakheet N. Z.
Published: 20/02/2026
Download PDF
Cite
x
APA
N. Z., N. Z. B. (2026). Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery, 7(1), 1-4.
MLA
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-4.
Chicago
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-4.
Harvard
N. Z., N. Z. B. (2026) 'Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-4.
Vancouver
N. Z. NZB. Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-4.
Download PDF
Research Article
Effect of Land Degradation on Livelihood
Kemalo Abdulmalik,
Isreal Zewide
Published: 04/01/2024
Download PDF
Cite
x
APA
Abdulmalik, K. & Zewide, I. (2024). Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery, 5(1), 1-4.
MLA
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-4.
Chicago
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-4.
Harvard
Abdulmalik, K. and Zewide, I. (2024) 'Effect of Land Degradation on Livelihood' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-4.
Vancouver
Abdulmalik K, Zewide I. Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-4.
Download PDF
Research Article
Gastric Cancer: A Comprehensive Review
Ali Shafeeq Neameh,
...
Hussein Riyadh Ali Shlaka
Published: 20/01/2026
Download PDF
Cite
x
APA
Neameh, A. S., Hatab, W. M. & Ali Shlaka, H. R. (2026). Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery, 7(1), 1-5.
MLA
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-5.
Chicago
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-5.
Harvard
Neameh, A. S., Hatab, W. M. and Ali Shlaka, H. R. (2026) 'Gastric Cancer: A Comprehensive Review' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-5.
Vancouver
Neameh AS, Hatab WM, Ali Shlaka HR. Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess
Asaad Mezher Hussain,
...
Mohammed Khazaal Hashim
Published: 31/12/2025
Download PDF
Cite
x
APA
Mezher Hussain, A., Jaber Abed, S. & Khazaal Hashim, M. (2025). Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery, 6(2), 1-6.
MLA
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6.2 (2025): 1-6.
Chicago
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6, no. 2 (2025): 1-6.
Harvard
Mezher Hussain, A., Jaber Abed, S. and Khazaal Hashim, M. (2025) 'Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess' Himalayan Journal of Medicine and Surgery 6(2), pp. 1-6.
Vancouver
Mezher Hussain A, Jaber Abed S, Khazaal Hashim M. Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery. 2025 Jul;6(2):1-6.
Srikumar, S., Muthiah, A. & Perumal, S. (2022). Role of Favipiravir Therapy in COVID 19 Patients A Systematic Review and Meta Analysis. Himalayan Journal of Medicine and Surgery, 3(1), 1-6.
MLA
Srikumar, Shabarini, Aravind Muthiah and Shridharan Perumal. "Role of Favipiravir Therapy in COVID 19 Patients A Systematic Review and Meta Analysis." Himalayan Journal of Medicine and Surgery 3.1 (2022): 1-6.
Chicago
Srikumar, Shabarini, Aravind Muthiah and Shridharan Perumal. "Role of Favipiravir Therapy in COVID 19 Patients A Systematic Review and Meta Analysis." Himalayan Journal of Medicine and Surgery 3, no. 1 (2022): 1-6.
Harvard
Srikumar, S., Muthiah, A. and Perumal, S. (2022) 'Role of Favipiravir Therapy in COVID 19 Patients A Systematic Review and Meta Analysis' Himalayan Journal of Medicine and Surgery 3(1), pp. 1-6.
Vancouver
Srikumar S, Muthiah A, Perumal S. Role of Favipiravir Therapy in COVID 19 Patients A Systematic Review and Meta Analysis. Himalayan Journal of Medicine and Surgery. 2022 Jan;3(1):1-6.