Mucositis is the breakdown of epithelial cells in the gastrointestinal tract. It is a common and painful side effect of treatment for many cancer patients. Oral cavity is a commonest site for mucositis however it can occur anywhere in the whole GI tract. Mucositis is very debilitating for patients and also lead to unwanted delays or dose reductions in life-saving treatments. Preventive strategies include good oral hygiene while treatment strategies mainly focus on the pain management. A stepwise treatment approach includes oral rinses, topical anaesthetics, and systemic analgesic agents.
Keywords
Oral Mucositis in Head and Neck Cancer Patients: A Review Article
Important Note:
Key findings:
The abstract highlights mucositis as a prevalent and painful side effect of cancer treatment, affecting the gastrointestinal tract's epithelial cells. It underscores the significance of preventive oral hygiene and stepwise treatment strategies, including oral rinses, topical anesthetics, and systemic analgesics, to manage symptoms and minimize treatment disruptions.
What is known and what is new?
Mucositis, common among cancer patients, affects the gastrointestinal tract's epithelial cells, predominantly in the oral cavity. While its debilitating nature and impact on treatment are known, the abstract emphasizes a comprehensive approach to management, highlighting preventive oral care and stepwise treatment strategies to alleviate pain and minimize treatment disruptions, potentially improving patient outcomes.
What is the implication, and what should change now?
Mucositis significantly impacts cancer patients' quality of life and treatment outcomes, often leading to treatment delays or modifications. Healthcare providers should prioritize preventive measures such as comprehensive oral care and adopt effective pain management strategies to alleviate patient suffering and ensure uninterrupted delivery of life-saving treatments, thereby improving overall treatment efficacy and patient well-being.
INTRODUCTION:
Oral mucositis (also known as inflammation of the oral mucosa) is a painful and debilitating side effect of cancer chemotherapy and radiotherapy (for patients with head and neck cancer). Oral mucositis is characterized by erythema, oedema, mucosal shedding, ulceration, and pseudomembrane formation. Severe symptoms can interrupt the delivery of treatment, increase the prolonged use of narcotics and antibiotics, increase the length of hospital stays, cause disruptions in eating (leading to the NG tube feeding), and increase the total cost of care [1-4].
Clinical features of mucositis and severity of mucositis in radiation patients are dose-dependent. After a cumulative dose of 10–20 Gy, hyperkeratinization occurs. After one week of therapy (>20 Gy ), patchy erythema results. After two to three weeks of therapy (or ~30 Gy), mucosal atrophy, ulceration, oedema, and even bleeding. Signs and symptoms persist until two to six weeks following the completion of therapy [5].
PATHOPHYSIOLOGY:
Traditionally, mucositis was believed to result from both direct and indirect toxicity to epithelial cells, interfering with the division and maturation of mucosal epithelial cells [6]. Direct mucositis was considered to be the direct damage that occurred to the rapidly dividing basal cell layers of the epithelium, resulting in clonogenic cell death, atrophy, and ulceration. Indirect toxic effects that lead to exacerbation of mucositis include the release of inflammatory mediators (that is, cytokines), granulocytopenia, and secondary infection [7].
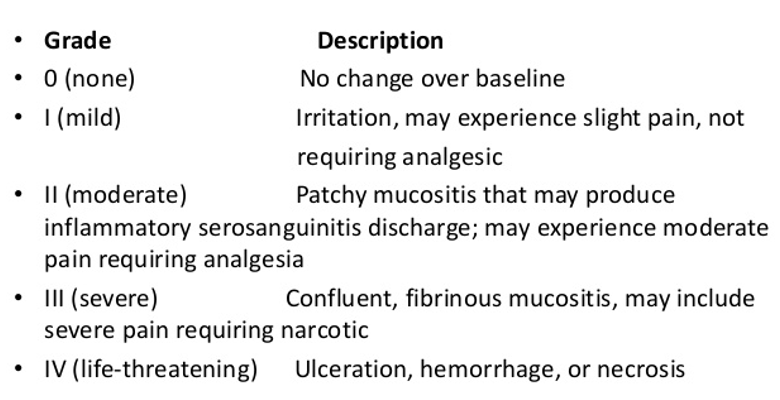
Oral mucositis is believed to involve five successive phases: initiation, message generation, signaling and amplification, ulceration, and healing. In the initiation phase, chemotherapy and radiotherapy generate reactive oxygen species (ROS), which damage cells, tissues, and blood vessels directly. This initiation leads to the next phases of message generation and signaling and amplification, in which secondary mediators of injury (such as nuclear factor kappa-B (NF-κB)) are stimulated. This stimulation leads to the up-regulation of genes that produce pro-inflammatory cytokines—such as tumour necrosis factor alpha (TNF-α), interleukin-1 beta (IL-1β), and interleukin-6 (IL-6)—which lead to additional tissue injury and apoptosis. Simultaneously, the pro-apoptotic ceramide pathway is activated, matrix metalloproteinase is up-regulated, fibronectin is broken down, and macrophages are activated. In the signaling and amplification phase, a series of positive feedback loops cause further up-regulation of the aforementioned inflammatory cytokines such as TNF-α and effector proteins induced in signaling pathways. These damaging events are concentrated in the submucosa and basal epithelium, resulting in a deceptively normal clinical appearance. When the basal epithelial cell layers experience sufficient injury and death, marked ulceration is observed, accompanied by profound pain and inflammation. The diagnosis of mucositis is generally based on clinical findings [8].
Figure 1: RTOG criteria for mucositis
Dentist's Role:
Dentists are involved in treating cancer patients, due to the role of oral hygiene in the prevention of oral mucositis and systemic infection. Dentists can provide preventative treatment prior to and during cancer therapy or provide direct treatment once mucositis is established. An initial dental prophylaxis must be done several weeks before the initiation of treatment; dental treatment must be completed at least one week before therapy begins. After the initiation of therapy, dentists must perform regular follow-up sessions.
Prevention:
With mucositis, as with all complications of cancer treatment, the goal is to prevent it from occurring.
Oral hygiene and care- Most preventive approaches focus on oral mucositis and generally include practicing good oral hygiene and keeping the mucosal area clean, dry, and free from possible sources of infection. Clinicians can prescribe oral rinses, such as bicarbonate or saline-containing products [9].
Cryotherapy- The theory behind oral cooling of the mouth is that the resulting vasoconstriction reduces blood flow to the epithelium, reducing the amount of chemotherapeutic drugs delivered to the mucosal cells [10, 11].
Antiseptic and antimicrobials- It prevents the colonization of potentially pathogenic bacteria, fungi, and viruses and prevents or lessens the severity of oral mucositis. Povidone-iodine is an antibacterial agent that has been shown to decrease radiotherapy-induced mucositis [12, 13].
Anti-inflammatories- Benzydamine inhibits the production of effects of inflammatory cytokines such as TNF-α and also have analgesic and anesthetic properties [3, 14-16].
Cytokines/growth factors- Granulocyte-macrophage colony-stimulating factor (GM-CSF) and granulocyte colony-stimulating factor (G-CSF) are hematopoietic growth factors that promote local accumulation of neutrophils in the mucosa and can induce endothelial and keratinocyte proliferation.
Palifermin, a recombinant human keratinocyte growth factor, induces epithelial cell proliferation, differentiation, and migration in normal epithelial tissue. When administered intravenously, palifermin has reduced the incidence and severity of oral mucositis in chemotherapy and stem cell transplant patients [17-20].
Parasympathomimetic- Saliva has both mucoprotective and antimicrobial effects that can prevent the incidence and severity of oral mucositis. Oral administration of pilocarpine is very useful in treating radiation-induced xerostomia. As parasympathomimetic, they increase secretion from exocrine glands (that is, sweat, salivary, lacrimal, gastric) [21, 22].
Treatment:
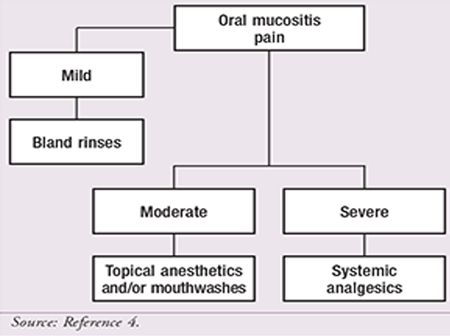
If mucositis does occur, the goal remains to keep the area clean and free from possible infectious sources. Therefore, oral rinses and antiviral or antifungal medications may still be used. In addition, changing all possible oral medications to IV forms to minimize patient discomfort. A bland, soft diet is recommended for oral mucositis patients. Acidic, spicy, salty, coarse, or dry foods should be avoided completely. (Figure 1)
The main focus of mucositis treatment should be adequate management of pain and palliation of symptoms. With this in mind, the National Comprehensive Cancer Network (NCCN) Task Force on Prevention and Management of Mucositis in Cancer Care suggests a stepwise approach for the treatment of mucositis pain.
Gabapentin- Another alternative for the treatment of mucositis pain in patients with head and neck cancer who are undergoing concomitant chemotherapy and radiation is gabapentin. It can be used for the treatment of neuropathic pain.
CONCLUSION:
Mucositis is a common and painful side effect of treatment for many cancer patients. Although preventive strategies and good oral hygiene are the key, the focus of treatment should be pain management. A stepwise approach is suggested based on NCCN findings. This strategy may include oral rinses, topical anaesthetics, and systemic analgesics. However, individual patient factors should be considered in the selection of appropriate pain-management strategies.
Funding: No funding sources.
Conflict of interest: None declared.
Ethical approval: The study was approved by the Institutional Ethics Committee of Indira Gandhi Medical College, Shimla.
Epstein, Joel B., and Mark M. Schubert. "Oropharyngeal mucositis in cancer therapy. Review of pathogenesis, diagnosis, and management." Oncology (Williston Park, NY) 17.12 (2003): 1767-79. https://europepmc.org/article/med/14723014
Epstein, Joel B., et al. "Prevention of oral mucositis in radiation therapy: a controlled study with benzydamine hydrochloride rinse." International Journal of Radiation Oncology* Biology* Physics 16.6 (1989): 1571-1575. https://doi.org/10.1016/0360-3016(89)90964-4
Laine, Pekka O., et al. "Oral infection as a reason for febrile episodes in lymphoma patients receiving cytostatic drugs." European Journal of Cancer Part B: Oral Oncology 28.2 (1992): 103-107. https://doi.org/10.1016/0964-1955(92)90036-Z
Spijkervet, F. K. L., et al. "Scoring irradiation mucositis in head and neck cancer patients." Journal of Oral Pathology & Medicine 18.3 (1989): 167-171. https://doi.org/10.1111/j.1600-0714.1989.tb00756.x
Lockhart, Peter B., and Stephen T. Sonis. "Alterations in the oral mucosa caused by chemotherapeutic agents. A histologic study." The Journal of dermatologic surgery and oncology 7.12 (1981): 1019-1025. https://doi.org/10.1111/j.1524-4725.1981.tb00208.x
Sonis, S. T., et al. "Defining mechanisms of action of interleukin-11 on the progression of radiation-induced oral mucositis in hamsters." Oral oncology 36.4 (2000): 373-381. https://doi.org/10.1016/S1368-8375(00)00012-9
Sonis, Stephen T., et al. "Perspectives on cancer therapy‐induced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients." Cancer: Interdisciplinary International Journal of the American Cancer Society 100.S9 (2004): 1995-2025. https://acsjournals.onlinelibrary.wiley.com/doi/abs/10.1002/cncr.20162
Cascinu, Stefano, et al. "Oral cooling (cryotherapy), an effective treatment for the prevention of 5-fluorouracil-induced stomatitis." European Journal of Cancer Part B: Oral Oncology 30.4 (1994): 234-236. https://doi.org/10.1016/0964-1955(94)90003-5
Adamietz, Irenäus A., et al. "Prophylaxis with povidone-iodine against induction of oral mucositis by radiochemotherapy." Supportive care in cancer 6 (1998): 373-377. https://link.springer.com/article/10.1007/s005200050179
Rahn, R., and I. A. Adamietz. "Mucositis in Patients during Antineoplastic Radiochemotherapy." Dermatology 195.2 (1997): 57-61. https://doi.org/10.1159/000246032
Prada, A., and F. Chiesa. "Effects of benzydamine on the oral mucositis during antineoplastic radiotherapy and/or intra-arterial chemotherapy." International journal of tissue reactions 9.2 (1987): 115-119. https://europepmc.org/article/med/3610509
Samaranayake, L. P., et al. "The effect of chlorhexidine and benzydamine mouthwashes on mucositis induced by therapeutic irradiation." Clinical Radiology 39.3 (1988): 291-294. https://doi.org/10.1016/S0009-9260(88)80538-5
Meropol, Neal J., et al. "Randomized phase I trial of recombinant human keratinocyte growth factor plus chemotherapy: potential role as mucosal protectant." Journal of Clinical Oncology 21.8 (2003): 1452-1458. https://doi.org/10.1200/JCO.2003.10.079
Spielberger, Ricardo, et al. "Palifermin for oral mucositis after intensive therapy for hematologic cancers." New England Journal of Medicine 351.25 (2004): 2590-2598. DOI: 10.1056/NEJMoa040125
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Applied Medical Sciences and Research open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Recommended Articles
Research Article
Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19
Aynar Talib Samad,
Yossra Saleh Khudhur
Published: 27/07/2021
Download PDF
Cite
x
APA
Talib Samad, A. & Khudhur, Y. S. (2021). Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19. Himalayan Journal of Applied Medical Sciences and Research, 2(2), 1-6.
MLA
Talib Samad, Aynar and Yossra Saleh Khudhur. "Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19." Himalayan Journal of Applied Medical Sciences and Research 2.2 (2021): 1-6.
Chicago
Talib Samad, Aynar and Yossra Saleh Khudhur. "Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19." Himalayan Journal of Applied Medical Sciences and Research 2, no. 2 (2021): 1-6.
Harvard
Talib Samad, A. and Khudhur, Y. S. (2021) 'Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19' Himalayan Journal of Applied Medical Sciences and Research 2(2), pp. 1-6.
Vancouver
Talib Samad A, Khudhur YS. Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19. Himalayan Journal of Applied Medical Sciences and Research. 2021 Jul;2(2):1-6.
Download PDF
Research Article
Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community
Vishal Dhatwalia,
Swati Chandel
Published: 10/12/2024
Download PDF
Cite
x
APA
Dhatwalia, V. & Chandel, S. (2024). Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research, 5(2), 1-5.
MLA
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5.2 (2024): 1-5.
Chicago
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5, no. 2 (2024): 1-5.
Harvard
Dhatwalia, V. and Chandel, S. (2024) 'Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community' Himalayan Journal of Applied Medical Sciences and Research 5(2), pp. 1-5.
Vancouver
Dhatwalia V, Chandel S. Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research. 2024 Jul;5(2):1-5.
Download PDF
Research Article
Infertility Insights: Exploring Knowledge of Causes and Treatments Among Women in Kangra, Himachal Pradesh
Priyanka Jamwal
Published: 20/12/2024
Download PDF
Cite
x
APA
Jamwal, P. (2024). Infertility Insights: Exploring Knowledge of Causes and Treatments Among Women in Kangra, Himachal Pradesh. Himalayan Journal of Applied Medical Sciences and Research, 5(2), 1-5.
MLA
Jamwal, Priyanka. "Infertility Insights: Exploring Knowledge of Causes and Treatments Among Women in Kangra, Himachal Pradesh." Himalayan Journal of Applied Medical Sciences and Research 5.2 (2024): 1-5.
Chicago
Jamwal, Priyanka. "Infertility Insights: Exploring Knowledge of Causes and Treatments Among Women in Kangra, Himachal Pradesh." Himalayan Journal of Applied Medical Sciences and Research 5, no. 2 (2024): 1-5.
Harvard
Jamwal, P. (2024) 'Infertility Insights: Exploring Knowledge of Causes and Treatments Among Women in Kangra, Himachal Pradesh' Himalayan Journal of Applied Medical Sciences and Research 5(2), pp. 1-5.
Vancouver
Jamwal P. Infertility Insights: Exploring Knowledge of Causes and Treatments Among Women in Kangra, Himachal Pradesh. Himalayan Journal of Applied Medical Sciences and Research. 2024 Jul;5(2):1-5.
Download PDF
Case Report
Mycosis Fungoides – A Case Report
Reema Bhatti,
...
Girija
Published: 20/10/2021
Download PDF
Cite
x
APA
Bhatti, R., Raina, D. & None, G. (2021). Mycosis Fungoides – A Case Report. Himalayan Journal of Applied Medical Sciences and Research, 2(2), 1-2.
MLA
Bhatti, Reema, Deepika Raina and Girija . "Mycosis Fungoides – A Case Report." Himalayan Journal of Applied Medical Sciences and Research 2.2 (2021): 1-2.
Chicago
Bhatti, Reema, Deepika Raina and Girija . "Mycosis Fungoides – A Case Report." Himalayan Journal of Applied Medical Sciences and Research 2, no. 2 (2021): 1-2.
Harvard
Bhatti, R., Raina, D. and None, G. (2021) 'Mycosis Fungoides – A Case Report' Himalayan Journal of Applied Medical Sciences and Research 2(2), pp. 1-2.
Vancouver
Bhatti R, Raina D, Girija G. Mycosis Fungoides – A Case Report. Himalayan Journal of Applied Medical Sciences and Research. 2021 Jul;2(2):1-2.
Bhatti, R. & Rohel, L. (2021). Oral Mucositis in Head and Neck Cancer Patients: A Review Article. Himalayan Journal of Applied Medical Sciences and Research, 2(2), 1-3.
MLA
Bhatti, Reema and Lovedeep Rohel. "Oral Mucositis in Head and Neck Cancer Patients: A Review Article." Himalayan Journal of Applied Medical Sciences and Research 2.2 (2021): 1-3.
Chicago
Bhatti, Reema and Lovedeep Rohel. "Oral Mucositis in Head and Neck Cancer Patients: A Review Article." Himalayan Journal of Applied Medical Sciences and Research 2, no. 2 (2021): 1-3.
Harvard
Bhatti, R. and Rohel, L. (2021) 'Oral Mucositis in Head and Neck Cancer Patients: A Review Article' Himalayan Journal of Applied Medical Sciences and Research 2(2), pp. 1-3.
Vancouver
Bhatti R, Rohel L. Oral Mucositis in Head and Neck Cancer Patients: A Review Article. Himalayan Journal of Applied Medical Sciences and Research. 2021 Jul;2(2):1-3.