This community-based cross-sectional survey provides an in-depth assessment of awareness, knowledge, and misconceptions regarding hypertension and its lifestyle risk factors among adults in Shimla district, Himachal Pradesh. The findings reveal that while a substantial proportion of respondents demonstrated good or very good knowledge, significant gaps persist—particularly in recognizing subtle symptoms, understanding preventive screening frequency, and addressing misconceptions about environmental and demographic risk patterns. These knowledge deficits are especially pronounced among older adults, rural residents, those with lower educational attainment, and individuals from lower-income households, underscoring the persistent health education divide within the district.
The overall knowledge distribution in our study—where 65% of participants achieved good or very good scores—compares favorably with several previous Indian studies, where awareness rates have often ranged between 40–60% in mixed urban–rural samples [13-16]. This relatively higher awareness in Shimla could be attributed to the district’s high literacy rate, penetration of mobile-based information channels, and increasing public health campaigns under the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS). Nevertheless, the fact that over one-third of participants fell into the fair or poor knowledge categories indicates that these campaigns have yet to achieve universal impact.
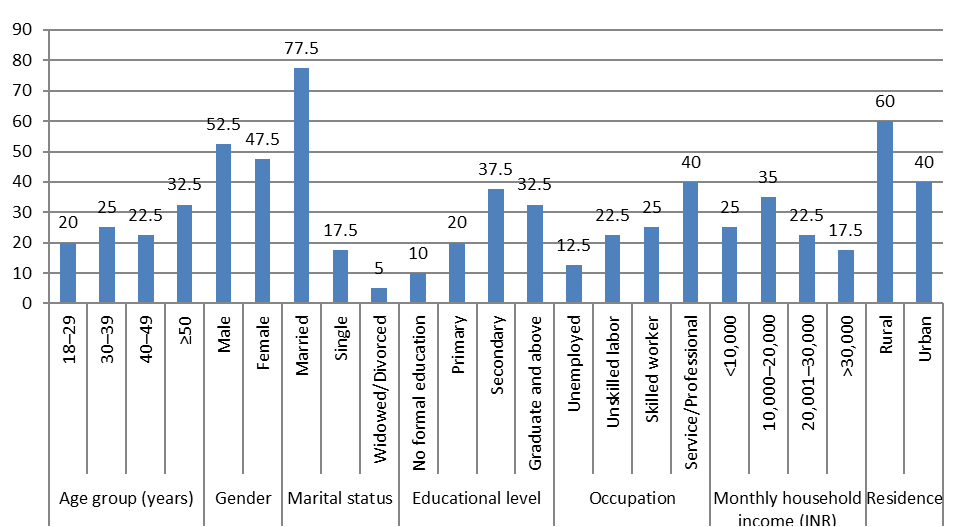
Our findings affirm the strong association between educational level and hypertension knowledge, consistent with prior studies, which have consistently shown that formal education enhances awareness of both non-communicable diseases and their lifestyle determinants [12-14]. Education not only improves comprehension of medical concepts but also facilitates access to and interpretation of health information from diverse sources, including digital media, print material, and healthcare providers. The occupational and income gradients observed in this study further reflect the socio-economic determinants of health literacy, wherein individuals in professional/service sectors and higher-income households are better positioned to access preventive health services and engage in informed lifestyle choices [14,15]
Rural–urban disparities, with urban residents outperforming rural participants in awareness scores, mirror patterns seen in other Indian hill states and national data [16-19]. This may be due to urban residents’ greater exposure to healthcare infrastructure, easier access to diagnostic facilities, and higher likelihood of encountering health promotion messages. However, rural populations—particularly in hilly regions like Shimla—face compounded challenges, including geographic isolation, limited specialist availability, seasonal accessibility issues, and cultural norms that may deprioritize preventive care. Targeted outreach in these communities, leveraging local health workers, Panchayat-led initiatives, and culturally relevant messaging, could bridge this gap.
Notably, the study uncovered specific conceptual weaknesses despite generally sound baseline awareness. For instance, only 57.3% correctly recognized that hypertension is more prevalent in urban settings, reflecting persistent misconceptions about rural immunity to lifestyle-related diseases. Similarly, less than two-thirds of respondents knew that annual blood pressure checks are recommended for healthy adults—a crucial gap given hypertension’s asymptomatic onset and the potential for early detection through routine screening. Symptom recognition was also limited; only 59.5% identified severe headache as a possible sign of dangerously high blood pressure, indicating that many individuals may underestimate or misattribute warning symptoms, delaying care-seeking.
Encouragingly, knowledge of key modifiable risk factors—such as high salt intake, physical inactivity, obesity, and excessive alcohol use—was relatively high, aligning with findings from previous studies [14,16,18]. This may reflect the increasing media coverage of lifestyle diseases and the integration of dietary advice into general health promotion campaigns. However, translating awareness into sustained behavioral change remains a critical challenge. Studies have shown that even among those aware of hypertension risks, adherence to low-salt diets, regular exercise, and weight control is often suboptimal, necessitating the integration of behavioral counseling and community-based support into public health strategies [17,19].
The association of younger age with higher knowledge scores in our study contrasts with findings from some Western populations, where older adults often report greater awareness due to more frequent health interactions.6,8,10 In India, however, younger cohorts—particularly those with higher education and internet access—may have greater exposure to online health information and social media campaigns. This generational shift in health information access presents an opportunity to harness youth engagement for intergenerational health promotion within households [17,19].
Our results reinforce the urgent need for context-specific, targeted educational interventions in Shimla. Mass media campaigns should be complemented by localized, interpersonal communication strategies, particularly in rural and low-literacy groups. Accredited Social Health Activists (ASHAs), Anganwadi workers, and community leaders could play pivotal roles in delivering consistent, culturally tailored messages. Furthermore, opportunistic blood pressure screening in community events, religious gatherings, and marketplaces could normalize preventive checks and address the gap in screening frequency awareness.
Strengths and Limitations
This study’s strengths include its relatively large and demographically diverse sample, use of a validated questionnaire, and exploration of multiple socio-demographic determinants of hypertension awareness. Conducting the survey via Google Forms enabled broad geographic reach across the district’s challenging terrain. However, certain limitations warrant consideration. The convenience sampling method may have introduced selection bias, as individuals with internet access and higher education levels may have been more likely to participate, potentially inflating overall awareness levels. Self-reported knowledge does not necessarily equate to healthy behaviors, and the cross-sectional design precludes causal inference. Moreover, while the questionnaire assessed awareness comprehensively, it did not evaluate actual blood pressure measurements, which would have provided insight into the relationship between awareness and hypertension prevalence.
Implications for Public Health Practice
These findings highlight the dual challenge of sustaining and enhancing existing awareness while closing the gaps among vulnerable groups. In Shimla, integrating hypertension education into routine primary care, school curricula, and workplace wellness programs could yield long-term benefits. Given the district’s unique geographical and cultural context, future interventions should also consider environmental factors such as altitude, seasonal work patterns, and dietary transitions. By aligning local initiatives with national frameworks like NPCDCS, and by prioritizing equity in health communication, Shimla can make significant strides in reducing the burden of uncontrolled hypertension and its complications.