Background: Acute Renal Injury(AKI) is a very common complication in critical patients [1]. The most recent guidelines state that Continuous Renal Replacement Therapy(CRRT) is the gold standard treatment in patients with severe AKI and hemodynamic instability, acute brain injury or increased intracranial pressure [2]. CRRT is, however, burdened by its high cost [3]. The present study was designed as observational and retrospective, and its objective was to calculate the costs and evaluate the effectiveness of CRRT in relation to the mortality outcome in Intensive Care Unit(ICU) and in the hospital 30 days after ICU discharge. Patients data were extracted from the “GiViTI–Italian Group for the evaluation of interventions in Intensive Care” database. All patients treated with CRRT in the years 2011-2014 in the Italian ICUs (189) and with a maximum SOFA score between 8 and 12, were enrolled (2599). Based on the SOFA Score, the expected mortality rate ranged between 22.5% and 48.5% [4]. We considered as unit cost the regional tariff (DRG) 3995.5 applied in the Perugia University hospital in 2015(€ 255.70). To get an approximation of the total cost for CRRT, the DRG was multiplied by the median duration of treatment (4 days) and the number of patients enrolled. The estimated total cost was € 2 658 257.20. The observed mortality in the ICU was 44.4%. The mortality rate 30 days after ICU discharge increased to 54.9% and was higher than predicted. Therefore, we suggest structuring a specific follow-up plan for patients who underwent CRRT in ICU as they have a higher mortality risk.
Keywords
Continuous Renal Replacement Therapy (CRRT)
INTRODUCTION
Nowadays, since there is an escalating demand for new services, which unfortunately coexists with constraints of new resources[5], the financial sustainability of the modern health care system is challenging. It is well known that the intensive care unit (ICU) is one of the hospital settings that absorbs most of the resources [6]. Recently, two group of authors tried to determine if the involvement of cost considerations in the ICU clinical decision-making could be useful [7-8]. Even if their position in this regard was opposite, they both concluded that results of health economics analysis are indeed valuable and, if correctly applied, they can bring benefits to the patients and the community, improving the quality of care.
Among the most frequent conditions in the ICU patients, severe acute kidney injury (AKI) is one of the most problematic; it increases morbidity, mortality and length of hospital stay [9], and its incidence has been rising in the last decades. The most recent guidelines state that CRRT is the gold standard treatment for patients with severe AKI and hemodynamic instability, acute brain injury or increased intracranial pressure [2]. However, this treatment is hindered by its high cost, which is due to the devices and the qualified professional staff needed [9].
Given these considerations, the objective of the present study was to evaluate the costs of continuous renal replacement therapy (CRRT)and its effectiveness in terms of mortality in patients with severe AKI.
MATERIALS AND METHODS
This study was designed as retrospective and multi-center. The goal was to calculate the costs of CRRT in critical patients and assess its effectiveness by confronting the ICU and the post-ICU outcomes with the mortality predicted by the SOFA Score.
Patients data have been extracted from the “GiViTI-Italian group for the evaluation of treatments in Intensive Care” database. All adult patients (age≥18) treated with CRRT in the participating ICUs (189) in the years 2011-2014, were enrolled. To increment the homogeneity of the cohort, a SOFA Score ranging from 8 to 12 was employed as an additional inclusion criterion. In the end, the study population comprised of 2599 patients.
To obtain an estimate of the total cost of CRRT, the regional tariff (DRG) 3995.5 (€ 255,70), applied in 2015 in the “Santa Maria della Misericordia” University hospital in Perugia, was employed. Subsequently, the DRG was multiplied by the median length of treatment (4 days) and the number of patients, to have an approximation of the resources needed to treat the study population.
To evaluate the effectiveness of CRRT, we tested if the actual outcomes were in line with the mortality predicted by the SOFA Score. Employing the findings from the study performed by Vincent et al. [4], we assumed that a SOFA Score between 8 and 12 predicted a risk of mortality ranging from 22,5% to 48,5%.The Fischer’s exact-test was used to compare the mortality rate during the ICU stay and the one 30 days after the discharge. A result of P<0.05 was considered significant. The statistical analysis was performed using GraphPad Prism software, version 7.02 for Windows [10].
RESULTS
Population characteristics
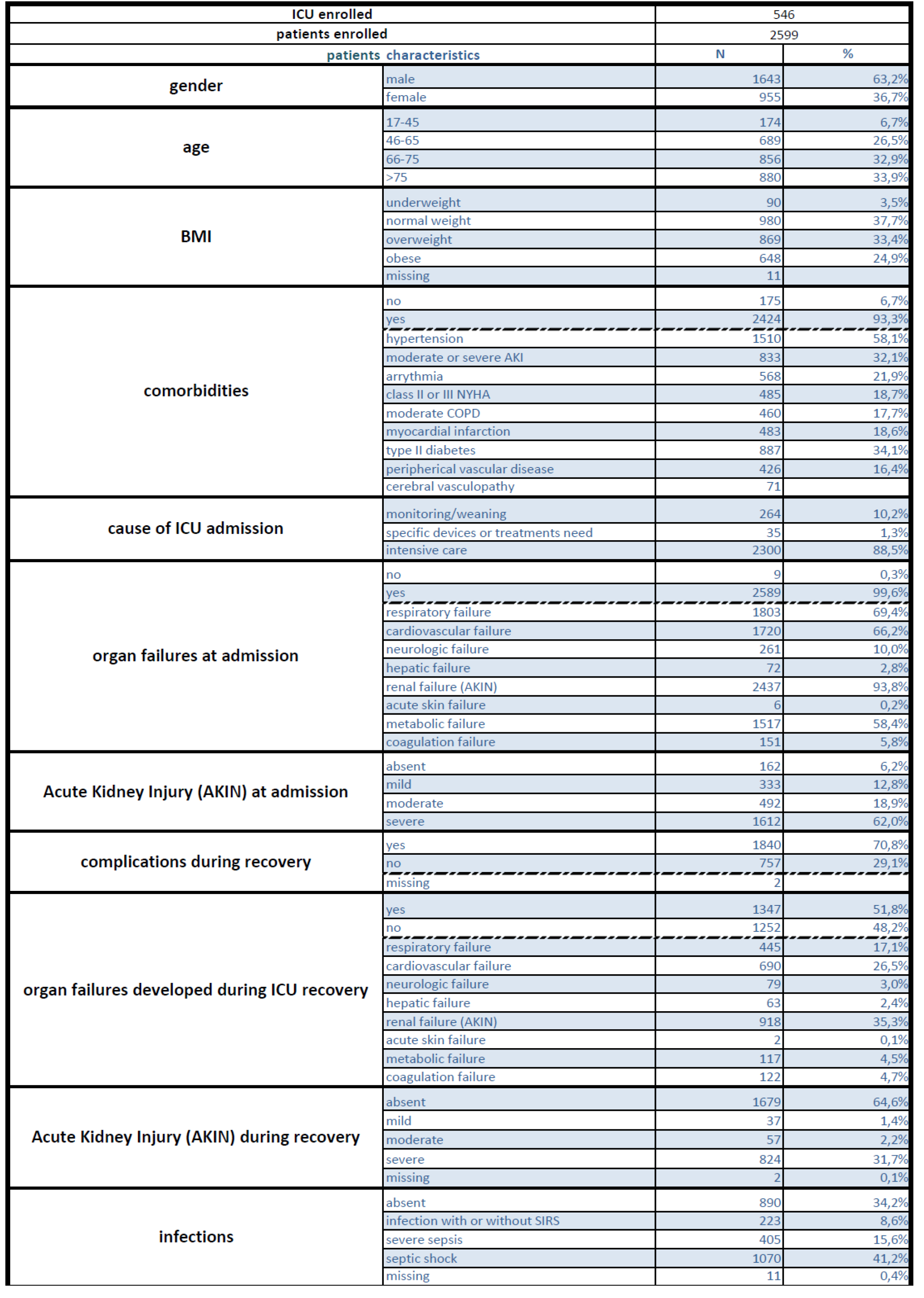
In the study cohort (Table 1), 63,2% of patients were males and 36,7% females, and their median age was 71. In most cases the BMI index classified them as normal (37,7%) or overweight (33,4%), whereas obese patients were 24,9% and underweight ones only 3,5%.
The reason for their admission to the ICU was almost always receiving intensive care; only 10,2% were checked in to be monitored or to be weaned from artificial ventilation, and 1,3% because they needed specific devices or treatments.
Comorbidities affected 93,3% of the population and, in terms of frequency, the top three were blood hypertension, type 2 Diabetes Mellitus and moderate or severe acute kidney injury.
At the moment of admission, organ failures were present in 99,6% of cases.
The AKIN criteria were employed to diagnose and classify renal impairment. According to them, severe AKI was present in 1612 patients, moderate AKI in 492 and mild AKI in 333.
During the ICU stay, complications occurred in 70,8% of cases and organ failures in 51,8%.
Endpoints
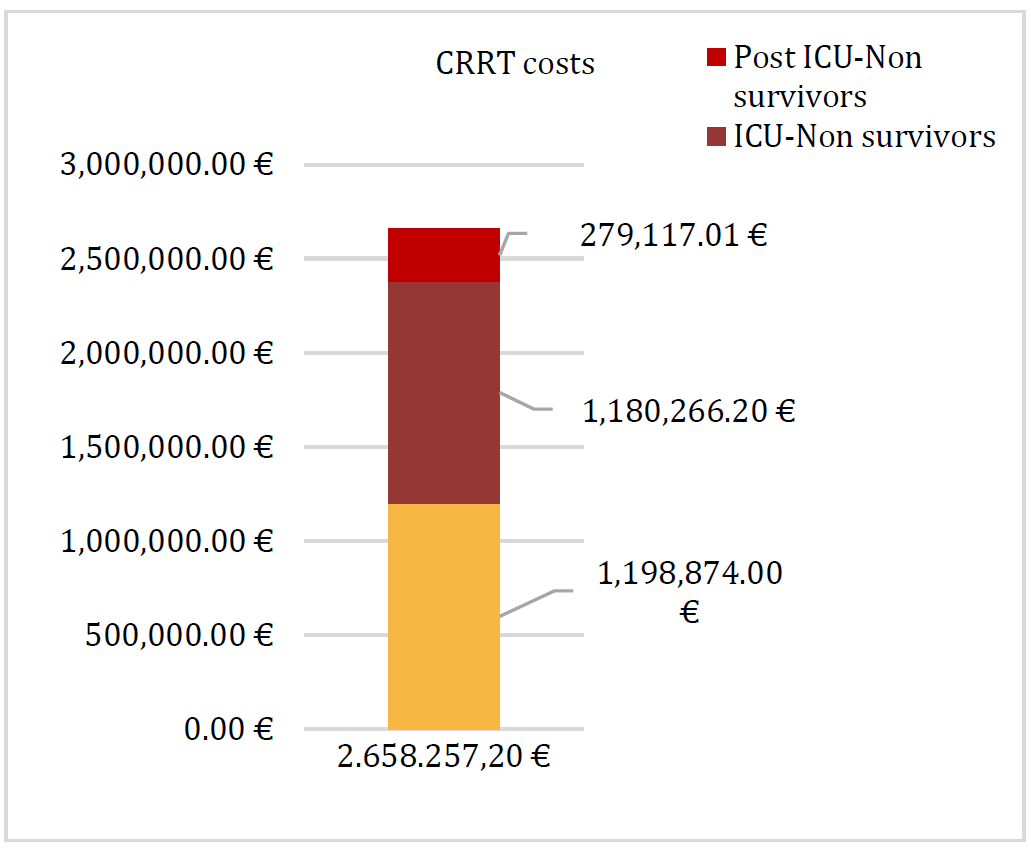
The estimated total cost of CRRT amounted to € 2 658 257,20.
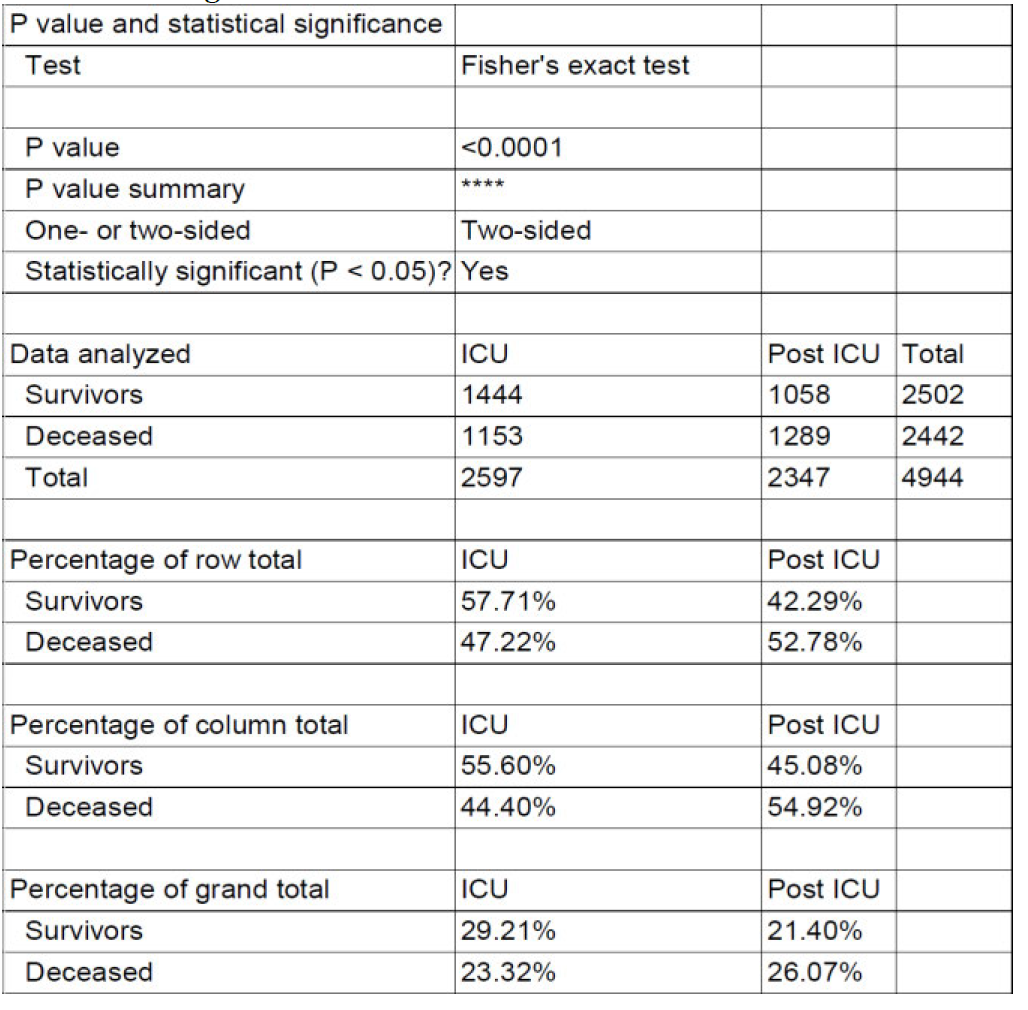
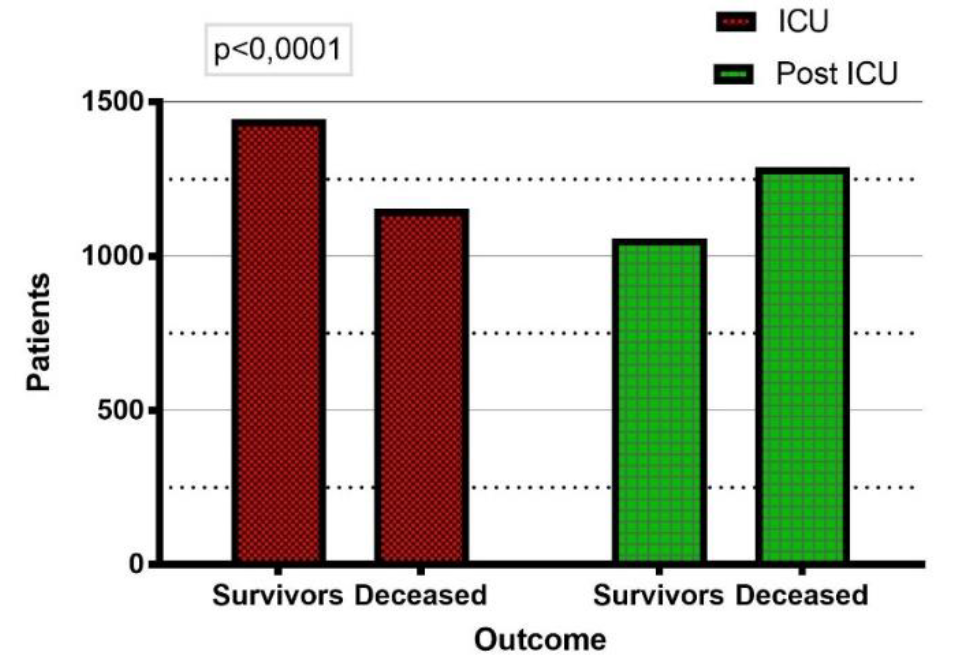
In the ICU, the mortality rate was 44,4%. An additional 10,5% of the population died in the hospital 30 days after ICU discharge; and the overall mortality rate was 54,9%. The Fischer’s exact-test proved that the difference in the outcomes was significant with a p<0,0001 (Table 2 Figure 1).
Analyzing this sum in regard to the patient’s mortality, we found that € 1 339 868 was spent for patients who survived 30 days after the ICU discharge, € 1 179 288, 40 for patients who died in the ICUs; and € 139 160,80 for patients who survived in the ICU, but then died in the hospital within the following 30 days (Figure 2).
DISCUSSION
The results of the present study indicate that the total cost of CRRT was estimated to be € 2.658.257,20. To obtain this estimate, we used the Perugia University hospital DRG, as we assumed it would be similar enough to the ones applied all over Italy, as these tools are developed with the aim to include all the real cost.
Additionally, we found that CRRT was effective in the ICU, where the mortality (44,4%) was in line with the prediction based on the SOFA Score (22-48,5%). However, this benefit vanished after 30 days of ICU discharge, because mortality increased by 10,5% and became higher than what was predicted.
The study was designed with the assumption that, if effective, CRRT should decrease the SOFA score and, with it, the mortality risk. In reality, this tool was initially conceived to describe organ impairment in septic patients, and our findings may be biased by an improper use of the score. However, SOFA has been found to relate well with mortality by several studies [11], andwe felt this was the most appropriate score to consider, as it has been studied both in the ICU and in the hospital wards [12-13]. Moreover, since AKI is usually precipitated and coexistent with other organ failures, it has been proven more predictive than other scores in critical patients with AKI [14]. So, we believe that, in these circumstances, SOFA was the most reliable score to predict both ICU and hospital short-term mortality. Ultimately, the present study is not the first one that used the SOFA score to evaluate the effectiveness of CRRT. In 2006, A. M. Rizal et al. already used the reduction of SOFA Score as unit of health interest and effective measure [15]. However, unlike our study, theirs was a single-center randomized clinical trial that aimed to compare high volume and standard dose emofiltration.
Conversely, to try to shed light on the reasons behind our results, it could be useful to consider what some recently published studies concluded. Fagugli et al. [16] reported that, despite the boost of AKI incidence in the University hospital “Santa Maria della Misericordia” in Perugia, the resources allocated to the Nephrology department did not increase accordingly. They observed that in the years 2007-2012 an escalating number of patients with severe AKI were treated in medical or surgical departments other than Nephrology, and that the opportunity to dispense them with appropriate treatment were limited. Moreover, Abraham et al. [17] concluded that in English hospitals where a Nephrology team was not present, 30 day mortality after AKI was significantly higher. Additionally, the UK National Confidential Enquiry into Patient Outcomes and Death (NCEPOD) Adding Insult to Injury AKI Study, reported in 2009 that only 50% of patients who died from a diagnosis of AKI received good care [18]. We feel probable that a suboptimal management of patients who developed AKI could be one of the reasons why CRRT effectiveness profile worsened after ICU discharge.
Our study has several limits, in addition to the obvious ones related to its retrospective design. It was not possible to carry out post-hoc analysis because the patients’ data extracted from the “GiViTI” database are aggregated. Nevertheless, we demonstrated that the difference in mortality during and after the ICU stay is significant.
Table 1: Baseline Demographics and Clinical Characteristics of ICU‑Enrolled Patients
Table 2: P Value And Statistical Significance Of Survivorship Outcomes During ICU And Post‑ICU Phases
Figure 1: Comparison of Survivors and Deceased Patients in ICU and Post‑ICU Phases (P < 0.0001)
Figure 2: Survival Outcome-Based Stratification of CRRT Costs in Critical Care Patients
In conclusion, AKI is a clinical condition whose treatment requires a significant use of resources in the Italian ICUs and hospitals. Moreover, 30 days after the ICU discharge the mortality rate of the study population increased and significantly exceeded the SOFA Score prediction. Therefore, as the human and wealth capital spent for CRRT is quite conspicuous, we suggest developing a specific follow-up program for patients with an increased mortality risk due to AKI. The identification of all these patients, who need specific care to help them “see the light”, may, at the same time, prevent enlarging the hospital “black hole” of negative outcome and wasteful use of resources.
REFERENCE
Uchino et al. “Acute renal failure in critically ill patients: a multinational, multicenter study.” JAMA, vol. 294, 2005, pp. 813–818.
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work. “KDIGO clinical practice guideline for acute kidney injury.” Kidney Int Suppl, vol. 2, 2012, pp. 1–138.
Klarenbach, S. et al. “Economic evaluation of continous renal replacment therapy in acute renal failure.” Int J Technol Assess Health Care, vol. 25, no. 3, 2009, pp. 331–338.
Vincent, J.L. et al. “Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study.” Crit Care Med, vol. 26, no. 11, 1998, pp. 1793–1800.
Goeree, R. et al. “Introduction to health economics and decision-making: is economics relevant for the front line clinician?” Best Pract Res Clin Gastroenterol, vol. 27, no. 6, 2013, pp. 831–844.
H.D.B. “CRRT in the area of cost containment: is it justified?” Am J Kidney Dis, vol. 30, 1997, pp. S102–S104.
Guidet, B. et al. “Should cost consideration be included in medical decisions? Yes.” Intensive Care Med, vol. 41, 2015, pp. 1839–1840.
Jeremy, B.D. et al. “Should cost considerations be included in medical decisions? No.” Intensive Care Med, vol. 41, 2015, pp. 1841–1843.
Klarenbach, S. et al. “Economic evaluation of continous renal replacment therapy in acute renal failure.” Int J Technol Assess Health Care, vol. 25, no. 3, 2009, pp. 331–338.
GraphPad Software Inc. “Prism 7.02 for Windows.” La Jolla, California, 2016.
Minne, L. et al. “Evaluation of SOFA-based models for predicting mortality in the ICU: a systematic review.” Crit Care, vol. 12, 2008, pp. R161.
Matsumura, Y. et al. “Serum procalcitonin level and SOFA score at discharge from the intensive care unit predict post-intensive care unit mortality: a prospective study.” PLoS One, vol. 9, no. 12, 2014, pp. e114007.
Mazzola et al. “The sequential organ failure score predicts 30 day mortality in a geriatric acute care setting.” J Gerontol A Biol Sci Med Sci, vol. 68, no. 10, 2013, pp. 1291–1295.
Chang, C.H. et al. “Acute kidney injury enhances outcome prediction ability of sequential organ failure assessment score in critically ill patients.” PLoS One, vol. 9, no. 10, 2014, pp. e109649.
Rizal, M. et al. “Cost-effectiveness analysis of continuous venovenous hemofiltration therapy in the treatment of sepsis in Hospital Universiti Kebangsaan Malaysia: a comparison between high volume and standard dose hemofiltration.” Malays J Community Health, vol. 12, 2006.
Fagugli, R.M. et al. “Six-year single-center survey on AKI requiring renal replacement therapy: epidemiology and health care organization aspects.” J Nephrol, vol. 28, 2015, pp. 339–349.
Abraham, K. et al. “Inequalities in outcomes of acute kidney injury in England.” QJM, vol. 105, 2012, pp. 729–740.
Stewart, J. “Adding insult to injury: care of patients with acute kidney injury.” Br J Hosp Med (Lond), vol. 70, no. 7, 2009, pp. 372–373.
Funding:
No funding sources
Ethical approval:
The study was approved by the University of Perugia
None
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Medicine and Surgery open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Advertisement
Recommended Articles
Research Article
Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori
Noor Zuhair Bakheet N. Z.
Published: 20/02/2026
Download PDF
Cite
x
APA
N. Z., N. Z. B. (2026). Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery, 7(1), 1-4.
MLA
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-4.
Chicago
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-4.
Harvard
N. Z., N. Z. B. (2026) 'Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-4.
Vancouver
N. Z. NZB. Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-4.
Download PDF
Research Article
Effect of Land Degradation on Livelihood
Kemalo Abdulmalik,
Isreal Zewide
Published: 04/01/2024
Download PDF
Cite
x
APA
Abdulmalik, K. & Zewide, I. (2024). Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery, 5(1), 1-4.
MLA
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-4.
Chicago
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-4.
Harvard
Abdulmalik, K. and Zewide, I. (2024) 'Effect of Land Degradation on Livelihood' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-4.
Vancouver
Abdulmalik K, Zewide I. Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-4.
Download PDF
Research Article
Gastric Cancer: A Comprehensive Review
Ali Shafeeq Neameh,
...
Hussein Riyadh Ali Shlaka
Published: 20/01/2026
Download PDF
Cite
x
APA
Neameh, A. S., Hatab, W. M. & Ali Shlaka, H. R. (2026). Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery, 7(1), 1-5.
MLA
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-5.
Chicago
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-5.
Harvard
Neameh, A. S., Hatab, W. M. and Ali Shlaka, H. R. (2026) 'Gastric Cancer: A Comprehensive Review' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-5.
Vancouver
Neameh AS, Hatab WM, Ali Shlaka HR. Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess
Asaad Mezher Hussain,
...
Mohammed Khazaal Hashim
Published: 31/12/2025
Download PDF
Cite
x
APA
Mezher Hussain, A., Jaber Abed, S. & Khazaal Hashim, M. (2025). Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery, 6(2), 1-6.
MLA
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6.2 (2025): 1-6.
Chicago
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6, no. 2 (2025): 1-6.
Harvard
Mezher Hussain, A., Jaber Abed, S. and Khazaal Hashim, M. (2025) 'Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess' Himalayan Journal of Medicine and Surgery 6(2), pp. 1-6.
Vancouver
Mezher Hussain A, Jaber Abed S, Khazaal Hashim M. Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery. 2025 Jul;6(2):1-6.
Nisi, F., Saviani, M., Galzerano, A. & Marturano, F. (2021). Continuous Renal Replacement Therapy (Crrt) in Critical and Post-Critical Patients: Wasteful Use of Resources or Actual Possibility of Survival?. Himalayan Journal of Medicine and Surgery, 2(1), 1-5.
MLA
Nisi, Fulvio, et al. "Continuous Renal Replacement Therapy (Crrt) in Critical and Post-Critical Patients: Wasteful Use of Resources or Actual Possibility of Survival?." Himalayan Journal of Medicine and Surgery 2.1 (2021): 1-5.
Chicago
Nisi, Fulvio, Michela Saviani, Antonio Galzerano and Federico Marturano. "Continuous Renal Replacement Therapy (Crrt) in Critical and Post-Critical Patients: Wasteful Use of Resources or Actual Possibility of Survival?." Himalayan Journal of Medicine and Surgery 2, no. 1 (2021): 1-5.
Harvard
Nisi, F., Saviani, M., Galzerano, A. and Marturano, F. (2021) 'Continuous Renal Replacement Therapy (Crrt) in Critical and Post-Critical Patients: Wasteful Use of Resources or Actual Possibility of Survival?' Himalayan Journal of Medicine and Surgery 2(1), pp. 1-5.
Vancouver
Nisi F, Saviani M, Galzerano A, Marturano F. Continuous Renal Replacement Therapy (Crrt) in Critical and Post-Critical Patients: Wasteful Use of Resources or Actual Possibility of Survival?. Himalayan Journal of Medicine and Surgery. 2021 Jan;2(1):1-5.