Introduction: Premature newborns with surgical conditions are at increased risk of morbidity and mortality due to their fragility and the immaturity of their organs. Our objective was to determine the prevalence of surgical conditions in premature infants, to identify them and to assess their morbidity and mortality. Method: This was a retrospective study carried out in the neonatology and pediatric surgery departments of the jeanne ebori foundation mother-child university hospital from January 2019 to October 2020. Results: During the study period, we collected 34 premature infants with surgical conditions. Premature infants accounted for 38, 2% of newborns with a surgical emergency. The prevalence of surgical emergencies in premature infants was 7.3%. The mean gestational age was 33 WA with extremes of 28 and 35+5 days WA. The sex ratio was 1. Digestive pathology represented 88, 2% of emergencies found. Abdominal wall emergencies accounted for 11, 8%. Neurological emergencies accounted for 8, 8%. 58, 8% of premature babies were operated on. The average time to surgical management was 5 days with extremes of 0 and 20 days. The average length of hospital stay was 17, 2 days with extremes of 1 and 69 days. The overall mortality was 50%. Postoperative mortality was 50%. Conclusion: The surgical emergencies of the premature newborn are represented in the foreground by the digestive affections. The improvement in their prognosis depends not only on the early diagnosis and treatment; but also the multidisciplinary collaboration between obstetricians, pediatrics surgeons and the neonatals resuscitators.
Keywords
Libreville Morbidity
Mortality
Prematurity
Surgical Emergencies
INTRODUCTION
A premature newborn is a newborn born before the end of 37 weeks of amenorrhea. It is immature and therefore fragile. Major premature surgery concerns complications of prematurity and congenital malformations. Surgery alone is a factor in morbidity and mortality. Also, the association between emergency surgery and prematurity constitutes a double factor of morbidity which further affects the prognosis. The absence of epidemiological data on surgery for premature babies in our country led us to conduct this study, the objective of which is to determine the prevalence of surgical conditions in this population at risk, to identify the various pathologies and to assess morbidity and mortality at the Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori (CHUMEFJE).
MATERIALS AND METHODS
Patients and Methods
We carried out a retrospective and descriptive study over a period of 2 years, from January 1, 2019 to December 31, 2020. The study took place in the neonatal medicine and pediatric surgery departments of the CHU Mère-Enfant Fondation Jeanne Ebori. It is a level 3 health structure located in the political capital Libreville whose hospital activity began on December 29, 2018. The neonatal medicine service has a capacity of 50 places. During this period, we included all premature babies having presented a surgical emergency, whether operated or not. The parameters studied in the newborn were: Gestational age (WA), birth weight, sex, different surgical pathologies, time to treatment, surgical treatment, length of hospitalization and evolution. Data were collected from patient medical records and operating room registers. They were entered and analyzed in Excel 2013.
This work has been reported in line with the STROCSS criteria [1].
RESULTS
During the study period 466 premature newborns were admitted to the neonatal medicine department of CHUMEFJE. The number of newborns who presented surgical emergencies was 89, including 34 premature newborns, i.e. a prevalence of 7.3% (n = 34/466) and 38.2% of all neonatal emergencies (n = 34/89).
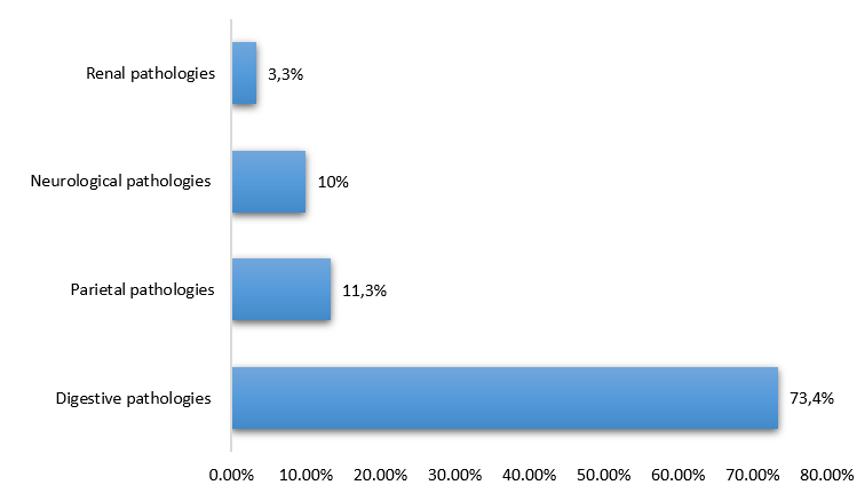
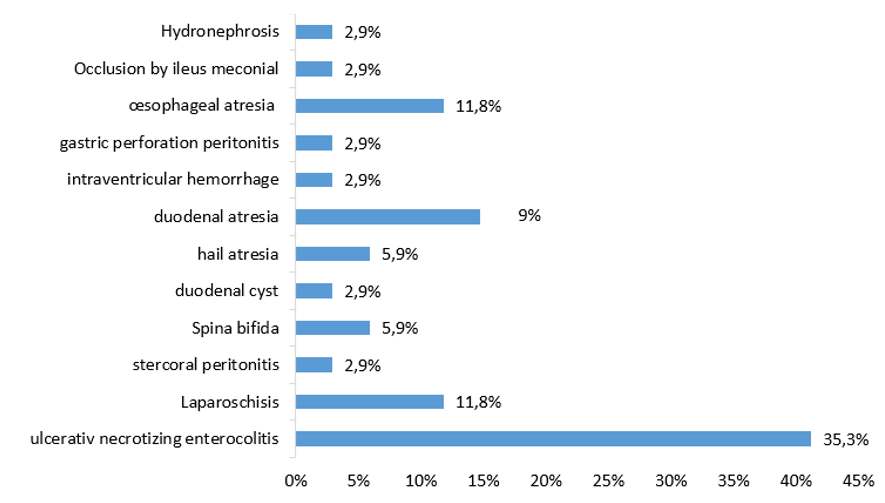
Surgical emergencies in premature newborns represented 12.4% of all surgical emergencies at CHUMEFJE. The mean maternal age was 28.1 years with extremes of 15 and 43 years. The mean gestational age was 32 weeks +3 days with extremes of 28 and 36 weeks + 6 days. The distribution of prematurity was 26.5% for extreme prematurity and 73.5% medium prematurity. The average weight was 1918.2gg with extremes of 600g and 4050g. The birth weight was less than 2500g in 85.3%, between 2500-4000 in 14.7%. Half of the newborns were male in with a sex ratio of 1 (Table I). Digestive pathologies represented 88.2% of surgical emergencies (Figure 1). Surgical pathologies were dominated by ulcerative necrotizing enterocolitis (41.2%) and duodenal atresias (Figure 2). Twenty out of thirty patients were operated on. The average time to surgical management was 5 days with extremes of 0 and 0 days. The average length of hospital stay was 8 days with extremes of 1 and 26 days. Overall mortality was 50%, dominated by ulcerative necrotizing enterocolitis (41.2%), esophageal atresia (23.5%). The mortality rate was the same after surgery or under medical treatment (50%) (Table 2).
DISCUSSION
The aim of this study was to determine the prevalence of surgical conditions in preterm infants and to assess their morbidity and mortality. The retrospective nature and the paucity of data in the literature on the subject somewhat limited our approach.
Nevertheless, we found a prevalence of 37% of premature newborns among total neonatal surgical emergencies. This is double the prevalence reported by Boumas et al. which found a prevalence of 19% [2]. This difference could be explained by the fact that the CHUME is currently and since its opening the reference center for mothers and children and that it brings together all of the country's pediatric surgeons.
The birth weight was less than 2500g in 85.3% Ndour [3] in Senegal found 53% of patients with a weight less than 2500g. the vulnerability of prematurity lies in its immaturity and low weight, which represents nearly three quarters of our sample.
Digestive emergencies represented 88.2% of the surgical conditions identified. This prevalence is well above those reported in Libreville (47.6%) Cocody (55%) and Yopougon (58.3%) [2,4,5]. Our study was specifically interested in the case of premature newborns who have the particularity of having immature organs, particularly in the digestive system.
Table 1: Newborn Parameters
Effectif (n)
(%)
Gestational age (WA)
Very preterm
9
26.5
Moderate preterm
25
73.5
Birth weight (g)
< 1500
9
26.5
1500-2500
19
55,9
> 2500
6
17,6
Sex (Sex-ratio=1)
Masculin
17
50
Féminin
17
50
Apgar
Apgar < 3
0
0
Apgar 4-6
4
11,8
Apgar ≥7
27
88,2
Table 2: Mortality by Type of Pathology
Pathologies
Number (n)
(%)
Ulcerative necrotizing enterocolitis
7
41,2
Oesophageal atresia
4
23,5
Duodenal atresia
2
11,8
Laparoschisis
1
5,9
Stercoral peritonitis
1
5,9
Gastric perforationperitonitis
1
5,9
Intraventricular hemorrhage
1
5,9
Figure 1: Breakdown of Surgical Pathologies by Device
Figure 2: Breakdown by Type of Pathology
Ulcerative necrotizing enterocolitis, which is a direct complication of prematurity, was the most frequently found surgical condition (41.2%). Schonnerr-hellec in Angers also states that ulcerative necrotizing enterocolitis is the most frequent medical and surgical emergency in premature infants [6].
The mean time to surgical management was 5 days, a delay also described by Ralahy and Takongmo [7,8]. In fact, in developed countries, antenatal diagnosis allows treatment from the first hours of life, which significantly improves the prognosis. Keita [9] in his series found 64.86% of newborns with more than 7 days of life on admission, he blames the ignorance of these pathologies by practitioners, the delay in diagnosis and home deliveries.
On the evolutionary level, we found an overall mortality of 50% and a postoperative mortality of 26.7%, Mieret in Ivory Coast found respectively 58.2% and 8.79%. The significant difference in postoperative mortality in our context could be explained by the selectivity of our sample on prematurity, but also by the delay in taking charge of the patient and finally by the inexperience of the staff in the treatment of these cases. patients. While Ouedraogo [10] in Burkina Faso describes 30.3% and 32.35%. In their context, postoperative mortality is still higher than that found at the CHUME.
In the sub-Saharan countries, mortality remains high, especially in Libreville in 2017 where it was 54.7% overall and 34.7% postoperatively, slightly above that which we found. In the DRC, on the other hand, overall mortality was lower, ie 43.3% [11]. This mortality can be explained by the delay in diagnosis and treatment, but also by the lack of the neonatal resuscitation technical platform in developing countries.
CONCLUSION
Surgical emergencies in premature newborns are dominated by digestive disorders, the first of which is ulcerative necrotizing enterocolitis.
The time taken to take charge is often long because of the diagnostic delay. Mortality is very high. A multidisciplinary collaboration between obstetrician gynecologists, neonatologists, pediatric surgeons and resuscitators would shorten the diagnostic time and would certainly improve treatment.
REFERENCES
Agha, R. et al. "The STROCSS 2019 guideline: Strengthening the reporting of cohort studies in surgery." International Journal of Surgery, vol. 72, no., 2019, pp. 156–165.
Boumas, N. et al. "Profil épidémiologique des urgences chirurgicales néonatales du chu de Libreville." Bull Med Owendo, vol. 15, no. 43, 2017, pp. 17–20.
Ndour, O. et al. "Facteurs de mortalité néonatale dans le service de chirurgie pédiatrique du chu Aristide le Dantec de Dakar." Le Mali médical, vol. 24, no. 1, 2009, pp. 33–38.
Midékor-Gonébo Kokoé, A. et al. "Les urgences chirurgicales néonatales dans le service de chirurgie pédiatrique du CHU de Cocody." Rev int sc méd-RISM, vol. 18, no. 2, 2016, pp. 161–164.
Mieret, J.C. et al. "Urgences chirurgicales néonatales dans le CHU de Yopougon." Annales des sciences de la santé, vol. 18, no. 1, 2018, pp. 1–5.
Schönherr-Hellec, S. et al. "Dysbiose et microbiote intestinal du nouveau-né prématuré : l’entérocolite ulcéro-nécrosante." Médecine thérapeutique / Pédiatrie, vol. 20, no. 3, 2017, pp. 188–195.
Ralahy, M. F. et al. "Mortalité néonatale au service des urgences du CHUA-JRA Antananarivo de Madagascar." Revue d’Anesth Réa et de Med d’Urgence, vol. 2, no. 1, 2010, pp. 15–17.
Takongmo, S. et al. "Les occlusions néonatales dans le service de chirurgie générale à Yaoundé." Med Afr Noire, vol. 47, no. 3, 2000, pp. 153–156.
Keita, M. et al. "Les urgences chirurgicales néonatales dans le service de chirurgie pédiatrique du Chu Donka." Le Mali médical, vol. 21, no. 4, 2006, pp. 16–20.
Ouédraogo, I. et al. "Epidémiologie des urgences chirurgicales néonatales à Ouagadougou." Archives de Pédiatrie, vol. 22, no. 2, 2015, pp. 130–134.
Cikomola Gulimwentuga, F. et al. "Les urgences chirurgicales néonatales à l’hôpital provincial général de référence de Bukavu en république démocratique du Congo." Pan African Medical Journal, vol. 24, no. 219, 2016, pp. 1–10.
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Medicine and Surgery open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Advertisement
Recommended Articles
Research Article
Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori
Noor Zuhair Bakheet N. Z.
Published: 20/02/2026
Download PDF
Cite
x
APA
N. Z., N. Z. B. (2026). Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery, 7(1), 1-4.
MLA
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-4.
Chicago
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-4.
Harvard
N. Z., N. Z. B. (2026) 'Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-4.
Vancouver
N. Z. NZB. Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-4.
Download PDF
Research Article
Effect of Land Degradation on Livelihood
Kemalo Abdulmalik,
Isreal Zewide
Published: 04/01/2024
Download PDF
Cite
x
APA
Abdulmalik, K. & Zewide, I. (2024). Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery, 5(1), 1-4.
MLA
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-4.
Chicago
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-4.
Harvard
Abdulmalik, K. and Zewide, I. (2024) 'Effect of Land Degradation on Livelihood' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-4.
Vancouver
Abdulmalik K, Zewide I. Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-4.
Download PDF
Research Article
Gastric Cancer: A Comprehensive Review
Ali Shafeeq Neameh,
...
Hussein Riyadh Ali Shlaka
Published: 20/01/2026
Download PDF
Cite
x
APA
Neameh, A. S., Hatab, W. M. & Ali Shlaka, H. R. (2026). Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery, 7(1), 1-5.
MLA
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-5.
Chicago
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-5.
Harvard
Neameh, A. S., Hatab, W. M. and Ali Shlaka, H. R. (2026) 'Gastric Cancer: A Comprehensive Review' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-5.
Vancouver
Neameh AS, Hatab WM, Ali Shlaka HR. Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess
Asaad Mezher Hussain,
...
Mohammed Khazaal Hashim
Published: 31/12/2025
Download PDF
Cite
x
APA
Mezher Hussain, A., Jaber Abed, S. & Khazaal Hashim, M. (2025). Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery, 6(2), 1-6.
MLA
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6.2 (2025): 1-6.
Chicago
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6, no. 2 (2025): 1-6.
Harvard
Mezher Hussain, A., Jaber Abed, S. and Khazaal Hashim, M. (2025) 'Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess' Himalayan Journal of Medicine and Surgery 6(2), pp. 1-6.
Vancouver
Mezher Hussain A, Jaber Abed S, Khazaal Hashim M. Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery. 2025 Jul;6(2):1-6.
Aboughe M., N., Mikolo A., L., Ndjotha B., N., M., A., E., C., Ntyale P., O., S.J., A. & Ndong F., O. (2021). Morbidity and Mortality of Surgical Emergencies in Premature Newborns: About 34 Cases. Himalayan Journal of Medicine and Surgery, 2(2), 1-3.
MLA
Aboughe M., Nkole, et al. "Morbidity and Mortality of Surgical Emergencies in Premature Newborns: About 34 Cases." Himalayan Journal of Medicine and Surgery 2.2 (2021): 1-3.
Chicago
Aboughe M., Nkole, Lembet Mikolo A., Nguele Ndjotha B., Abeghe M., Comlan E., Orema Ntyale P., Ategbo S.J. and Ondo Ndong F.. "Morbidity and Mortality of Surgical Emergencies in Premature Newborns: About 34 Cases." Himalayan Journal of Medicine and Surgery 2, no. 2 (2021): 1-3.
Harvard
Aboughe M., N., Mikolo A., L., Ndjotha B., N., M., A., E., C., Ntyale P., O., S.J., A. and Ndong F., O. (2021) 'Morbidity and Mortality of Surgical Emergencies in Premature Newborns: About 34 Cases' Himalayan Journal of Medicine and Surgery 2(2), pp. 1-3.
Vancouver
Aboughe M. N, Mikolo A. L, Ndjotha B. N, M. A, E. C, Ntyale P. O, S.J. A, Ndong F. O. Morbidity and Mortality of Surgical Emergencies in Premature Newborns: About 34 Cases. Himalayan Journal of Medicine and Surgery. 2021 Jul;2(2):1-3.