Cholecystoenteric fistula is an abnormal communication between the gallbladder and the gastrointestinal tract. It is a rare complication of cholelithiasis [1]. The cholecystoenteric fistula presents in variable symptoms and an accurate diagnosis before surgery is rare [2]. Here, we report a case that was preoperatively thought of as cholelithiasis with choledocholithiasis but intraoperatively, a cholecystoduodenal fistula with impacted CBD stones was seen.
Case Report
A 55 years old lady presented with pain in the right upper abdomen and nausea since one month. The pain was intermittent, non-radiating with no aggravating factors and relieved with medications. There was no associated fever, jaundice, hematemesis, or melena. There was no previous abdominal surgery. The patient was hypertensive and diabetic, both of which were under control with oral medications. She had no known allergies or addictions.
Examination of the patient revealed a tender right upper abdomen with mild hepatomegaly. There were no other findings.
We thus set out to work up the patient with some blood investigations and an ultrasound of the abdomen.
The hemoglobin was 13.8 g/dL, the total leucocyte count was 7,700/mm3 and the platelets were 1.83 lakh/mm3. The renal function test was normal.
The liver function test revealed that total Bilirubin was 0.5 mg/dL, SGPT was 79 U/l, SGOT was 62 U/l and alkaline phosphatase was 68 IU/l.
The ultrasound of the abdomen showed that the liver had increased reflectivity. The biliary channels were normal. The gall bladder was contracted and had few echogenic foci in the lumen, the largest of which was 9.3mm. The wall thickness was 3.6mm. CBD was dilated (7.9mm) and showed echogenic foci of 8.1mm in the lumen. It gave the impression of cholelithiasis with choledocholithiasis and associated Grade I Fatty Liver (Figure 1).
Given the CBD stones, an MRCP was done. It showed a contracted gall bladder with small intra-luminal filling defects. Intrahepatic biliary radicals were not dilated, but the right and left hepatic ducts were prominent. CBD was dilated with a maximum diameter of 8.4mm. Intra-luminal filling defects were seen in mid-CBD, the largest one being 8.1 mm.
A provisional diagnosis of choledocholithiasis and cholelithiasis was made and the patient was put up for ERCP. In ERCP, selective cannulation of the CBD was done.


Figure 1: USG showing gallstones and dilated CBD stones
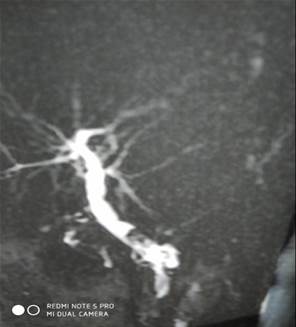
Figure 2: MRCP showing dilated CBD and filling defects

Figure 3: Postoperative Specimen of the gall bladder and the stones
The CBD had a doubtful filling defect. We proceeded with a wire-guided sphincterotomy and balloon sweeping. Balloon sweeping yielded sludge. A 10 Fr 5 cm stent was placed inside the CBD at the end of the procedure (Figure 2).
The patient was put up for laparoscopic cholecystectomy after 2 days. Intraoperatively, adhesions between the gall bladder and omentum were seen. Once the adhesions were separated the gall bladder was visualized which was contracted and very small. Surprisingly, a fistulous tract was seen coming from the gall bladder to the first part of the duodenum. It was dissected out. It was proposed to apply a laparoscopic stapler over the fistulous tract and proceed, but due to the dense adhesions and difficult anatomy, it was decided to convert it into a laparotomy.
On opening, it was found that the gall bladder was very small (about 1.5cm) without any stone or mass. The fistulous tract between the GB The fistula could have been dealt with a laparoscopic stapler device but as the CBD anatomy was not clear it was deemed wise to convert to an open procedure. and 1st part of the duodenum was confirmed. It was excised and the duodenal opening was repaired with 2/0 Vicryl with an Omental patch over it. A standard cholecystectomy was subsequently done.
On inspecting the CBD, it was found dilated. Palpation of the CBD revealed two stones at the lower end. The stent was also palpable inside. On opening the CBD, the stent was seen, but the stones were not appreciated. The stent was removed but still no stones were seen. Then the tissue over the stones was incised and two stones (1 cm and 5 mm approx) were removed. After thorough saline irrigation, as sphincterotomy had been done previously, the CBD was closed primarily after placing a plastic stent. The abdomen was closed with a drain at Morrison's pouch.
The post-operative period was uneventful. The patient was discharged on day 7 with advice for removal of stitches locally and to come for endoscopic stent removal after 1 month (Figure 3). On the 20th day, the patient called to inform us that a tube-like thing had passed with stool. The patient was reassured and was advised for doing LFT which came out to be normal. The patient is on follow-up and is asymptomatic.


