Interstitial Lung Disease (ILD) defines any disease that affects the interstitium and the distal alveoli of the lungs, leading to impaired lung diffusion. It is a heterogeneous group of different diseases of unknown and known cause with common functional characteristics (restrictive physiology and impaired gas exchange) and a common final pathway, eventually leading to irreversible fibrosis [1,2,3].
Although well over 100 distinct entities of ILDs are recognized, a limited number of disorders, including idiopathic pulmonary fibrosis, sarcoidosis and connective tissue disease-related ILDs, account for most ILDs encountered clinically [4].
Some factors have been identified to be associated with poorer prognosis and shorter survival time among ILDs patients are older age, smoking status (smokers and ex-smokers), lower body mass index, more impaired pulmonary function (mainly on forced vital capacity, FVC, total lung capacity, TLC and diffusing capacity for carbon monoxide, DLCO), radiological findings (usual interstitial pneumonia, UIP), a pattern or greater extent of fibrosis and the development of acute exacerbations or comorbidities, especially pulmonary hypertension and emphysema [5].
Little is known on the characteristics of patients diagnosed with idiopathic pulmonary fibrosis (IPF) in this hilly area of northern India. The present study was done to evaluate the Socio-demographic and etiological profile of Interstitial Lung Diseases (ILDs) patients.
Aims and Objectives
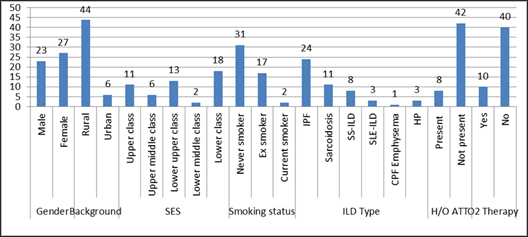
To study the Socio-demographic and etiological profile of Interstitial Lung Diseases (ILDs) patients.