The liver and the spleen, although they relatively protected by the inferior ribs, represent commonly injured organs during abdominal blunt trauma, accounting for about two-thirds of all visceral injuries [11]. Abdominal CT scan is an essential modality for the accurate diagnosis and grading of liver injuries in hemodynamically stable cases and is considered useful to guiding the management approach [12]. In addition to injury grading, it detects active bleeding (i.e., blush, contrast extravasation and venous phase), pseudoaneurysm which is a common cause of failure to non-surgical management and associated intraperitoneal injuries and also it quantifies the associated haemoperitoneum [13]. This change in the management has many potential benefits, as early hospital discharge, cost-effectiveness and decreasing of nontherapeutic laparotomies, intra-abdominal complications and the need for blood transfusion [14].
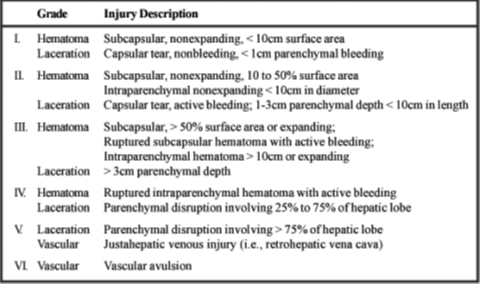
In this study, the most common mechanism of injury was Road Traffic Accident (RTA) (62.9%). Regarding associated injury, 56.5% had associated chest injury and 41.9% of them had associated head injury. Concerning grade of liver injury, it was graded II in 29% and graded I and III in 25.8% of study patients. Regarding associated injury, 56.5% had associated chest injury and 41.9% of them had associated head injury.
In Al-Diwaniya/Iraq, Handoz and colleagues in a study conducted in 2017, found that RTA was the commonest cause for blunt liver trauma, as found in 40%, followed by fall from height or stairs in 20% of participants. The grades of liver injury assessed by CT findings were; grade I in 60%, grade II in 30%, grade III in 10%. The associated chest injuries were most common followed by head injury [15]. In comparison to other studies, Brillantino et al. study in Italy 2019, found that commonest cause of blunt liver injury was RTA (56.9%). According to AAST organ injury scale, 34.8% of patients had grade I, while 26.5% had grade II and only 5.5% of them had grade V injuries. About 86.8% of patients showed multiple injuries, the more frequent lesions were rib fractures, observed in 70.1% of cases, followed by long bones fractures in 34.8% and head or maxillofacial injuries in 14.3% of cases [16].
Another Iraqi study which has been conducted in Baghdad 2017 by Al-Aubaidi and other authors, in which 38.33% of patients presented with grade II liver injury making it the most commonly encountered grade of injury while 31.67% of patients had grade III as second most common grade of injury. Diaphragmatic injury was the most common associated organ injury with liver injury in 50% of patients [17].
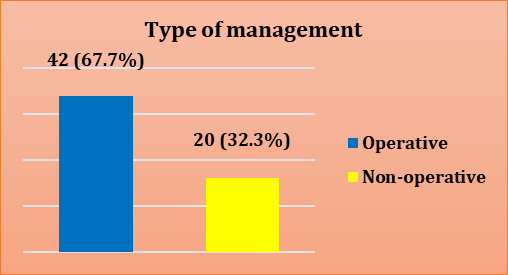
In the current study, more than two thirds of study patients (67.7%) were managed by surgical intervention; while 32.3% of them were treated conservatively, in contrast to Brillantino et al. study whereby only (14.6%) OF patients underwent operative management. The indications for surgery were the presence of persisting hemodynamic instability despite fluid therapy, peritonitis and thoraco abdominal injuries [16], another different result reported by Kaptanoglu and colleagues in their study in Turkey 2017, in which 300 injured patients enrolled, of them 192 patients (64%) were observed conservatively, while 108 cases (36%) received abdominal surgery [18], which was lower than present study. This difference could be due to different facilities for diagnosis and management available in our hospital compared to other hospitals in other countries as well as the different sample size, the causative factor and severity of liver injury may also contribute to the different results.
In operative group of this study, 33.3% complained from wound infection; which was the commonest complication, while in non-operative group, 10% complained from ongoing bleeding.
A different finding observed in Afifi et al study in Qatar 2018, they noticed that overall complications were pneumonia (16.7%), sepsis (10.1%) and RDS (3.5%), which frequently associated in-hospital complications. Specific complications of liver injury per say include biloma in 1% and 1.5% developed pseudoaneurysm on the conservative group, massive liver necrosis occurred in 0.5% of patient after angioembolization [19]. The different results could be due to different modalities of treatment that is adopted by them and different sample size which was 257 patients over 3 years.
In Iraq also, Al-Aubaidi et al. study in Iraq 2017 noticed in concern to postoperative complications, that wound infection was the commonest postoperative complication in 13.33% of patients followed by respiratory complications (10%), jaundice (8.33%), bile leak (5%), subphrenic collection (5%), DIC (5%), bleeding (3.33%), hemobilia (1.67%) and liver abscess and necrosis (1.67%) [17].
In the current study, 6.5% of patients died and all of them were from the operative group. This rate was close to that observed in Afifi et al. study in Qatar 2018, as reported that 20 of 257 injured patients died (7.8%) (19). The overall mortality in Fodor et al. study in 2019 study was 4.8%, with 11% in the surgery group and 3.5% in non-operative management group [20], this result was in line with other published data conducted by Ghnnam and other co-authors in Saudi Arabia, in which they noticed that overall mortality rates around 3.5% [21]. A higher result observed in Kaptanoglu et al. study in Turkey 2017, in which 13% of injured participant died and the main determinants of mortality were hemodynamic instability on admission.
This study revealed that prevalence of operative option of management was increasing with increasing grade of liver injury to reach 100% in patients with grade V liver injury with a significant association (p = 0.003) between type of management and grade of liver injury, while no statistically significant association with mechanism of injury and all types of associated injuries (p>0.05) [18]. The same results obtained in Afifi et al study in Qatar 2018, in which the highest grade of injury was treated operatively with significant correlation between type of management and grade of injury exist (p<0.001) [19]. Another agreement noticed in Ghannam et al study in Saudi Arabia 2013, as reported that patients treated operatively, had a higher grade of liver trauma. Grading of injury showed significant difference with the type of management (p<0.001) [21].
In this study, mean of duration of hospitalization was significantly higher in patients who managed surgically than that in those who managed conservatively (p = 0.001).
In Saleh et al study in Egypt 2016, 27 patients treated with non -operative management (79.42 %) were discharged within 1 week, 7 patients (20.58 %) were discharged within 1–2 weeks of admission but no patient stayed for more than 2 weeks. The mean hospital stay in non-operative management was 7.5 days, while 12 patients treated with operative management (46 %) were discharged within 1 week, 11 patients (42 %) were discharged within 1–2 weeks of admission and no patient stayed for more than 2 weeks [22].
The advantages of non-operative management for blunt liver injury may encourage more surgeons to adopt, whenever possible to decrease the complications of the old strategy that encourage the operative management.