Method of Management, Complications and Patient Satisfaction Among Obstetrics and Non-Obstetrics Patients Having Post Dural Puncture Headache (Pdph) After Undergoing Surgeries Under Subarachnoid Block in a Tertiary Care Hospital
C.M. Negi
1
,
Poonam
2
,
Mast Ram
3
1
Department of Anaesthesiology, Regional hospital, Reckong Peo, Kinnau, H.P., India
2
Department of Anaesthesiology, Civil Hospital, Tauni Devi, Hamirpur, H.P., India
3
Department of General Surgery, Civil Hospital, Rajgarh, Sirmour, H.P., India
Background: The present observational study was carried out to evaluate the method of Management, Complications and Patient satisfaction among obstetrics and non-obstetrics patients having Post Dural Puncture Headache (PDPH) after undergoing surgeries under subarachnoid block in a Tertiary Care Hospital. Material and Methods: This was a observational Prospective study carried out at Department of Anaesthesia, Dr Rajendra Prasad Medical College, Tanda conducted on consecutive patients ASA I and II, aged 20-60 years, obstetric/ non obstetric patients scheduled for surgery under subarachnoid block, over a period of 18 months including data collection, data organization, presentation, analysis and interpretation.After recruitment, the patients were divided into two groups comprising of obstetric and non-obstetric group. Results: The total patients included were 302, being 115 in obstetric group and 187 in non-obstetric group. In our study, out of 302 patients only 17 patients had post dural puncture headache, the total incidence being 5.6%.There were eight (7%) patients in obstetric and nine (4.8%) patients in non-obstetric group. All patients with PDPH had resolution of their symptoms by conservative management (hydration, bed rest, acetaminophen and NSAIDS), the PDPH resolved in 2(25%) of the parturients within the 1st day of its commencement, 5 (62.5%)parturients and 4 patients (44.4%) in non obstetric group had relief 2nd day after commencement of the headache. Whereas, one parturient(12.5%) and 4 patients(44.4%) in non obstetric group got relief on the 3rd day. One patient in non obstetric group (11.1%) had relief on the fourth day. 29% of the patient responded to the fluid and bed rest, whereas 35.2% patients required acetaminophen tablet as well, however 35.2% patients required the non steroidal anti-inflammatory drugs as well. No patient in either group required epidural blood patch. In obstetrics and non-obstetrics population, incidence of nausea and vomiting was in 8.7% and 7.5% patients respectively.Other complications like backache, vertigo were 2.61% and 2.7% patients in obstetric and non-obstetric population respectively. In obstetrics and non-obstetrics population, patient satisfaction was comparable (P=0.0778). Conclusion: All patients with PDPH had resolution of their symptoms by conservative management (hydration, bed rest, acetaminophen and NSAIDS) within 3-4 days while incidence of nausea and vomiting and other complications like backache, vertigo were very less.
Keywords
Evaluation
Method of Management
Complications
Patient Satisfaction
Post Dural Puncture Headache (PDPH)
Subarachnoid Block
INTRODUCTION
The role of spinal anaesthesia for caesarean section is well established because of its safety, low cost and reliability.However the spinal anaesthesia especially in obstetrics is associated with increased incidence of post dural puncture headache (PDPH) leading to prolonged hospital stay, increased morbidity and therefore decreased preference to subarachnoid block in the subsequent pregnancies [1-2].
According to the Headache Classification Committee of the International Headache Society, headache after lumbar puncture is defined as “bilateral headaches that develop within 7 days after a lumbar puncture and disappears within 14 days. The headache worsens within 15 min of resuming the upright position, disappears or improves within 30 min of resuming the recumbent position.”Post dural puncture headache causes considerable morbidity and is a complication that should not to be treated lightly. The relatively high incidence of post dural puncture headache in the obstetric patients is a major disadvantage of subarachnoid block [3-4].
Recently, in the national inpatient database study [5] the authors observed the incidence and risk factors for post dural puncture headache after neuraxial anaesthesia in obstetric vs non obstetric patients, retrospectively by collecting the data from nationwide inpatient administrative claims and discharge database. This study has been planned to evaluate the method of Management, Complications and Patient satisfaction among obstetrics and non-obstetrics patients having Post Dural Puncture Headache (PDPH) after undergoing surgeries under subarachnoid block in a Tertiary Care Hospital
Aim and Objectives
To evaluate the method of Management, Complications and Patient satisfaction among obstetrics and non-obstetrics patients having Post Dural Puncture Headache (PDPH) after undergoing surgeries under subarachnoid block in a Tertiary Care Hospital
MATERIALS AND METHODS
Study Design: An Observational Prospective study
Study area: The study was carried out at Department of Anaesthesia, Dr Rajendra Prasad Medical College, Tanda
Study population: After obtaining approval from Institution Ethics Committee, this observational study was conducted on consecutive ASA I and II, aged 20-60 years, obstetric/ non obstetric patients scheduled for surgery under subarachnoid block, over a period of 18 months
Study duration: This study was conducted over a period of 18 months including data collection, data organization, presentation, analysis and interpretation
Inclusion Criteria: Non obstetric patients /parturients belonging to age group of 20 to 60 yrs, ASA physical status I, II scheduled for surgery under spinal anaesthesia were included
Exclusion Criteria: Patients presenting with fetal distress, toxemia of pregnancy, CVS/CNS disorders, neuromuscular diseases (eg, myopathies and neuropathies), hypovolemia, acid base disturbances and electrolyte imbalance, obese, infection on the back, on anticoagulant therapy and vertebral anomaly were excluded from the study
Study Tools: Semi structured Performa containing demographic profile of study population and preoperative parameters in relation to objectives of the study
Methodology
Preoperative evaluation included detailed history, general and spine examination, routine laboratory investigations. All patients received gastric aspiration prophylaxis. In the operating room, 3-lead ECG, noninvasive blood pressure and pulse oximetry were attached and parameters recorded.
A good intravenous access was established. After recording baseline vital parameters parturients/patients were preloaded with 500-1000mL of crystalloid solution. Standardized anaesthetic technique was employed for every patient.The attending anaesthetist was free to choose the type of spinal needle (however in our institution we used 26 G quincke spinal needle because of availability), approach (median/ paramedian), dose of intrathecal drug, position for spinal.
After about five minutes, level of block (sensory, motor) was assessed. Surgeons were asked to proceed for surgery after adequate block to T5 is confirmed using pin prick for sensory and bromage scale for assessment of motor blockade. Demographic details of each patient were filled in the study questionnaire during the procedure.
The patients were assessed for hemodynamic variables ie heart rate, systolic, diastolic and mean blood pressure and percentile of oxygen saturation every three minutes till the end of the procedure. The patient was then followed up by another anaesthetist who was blinded to the patient and the size of the needle and the number of punctures. The patient was followed up in the day one and upto three days with regards to PDPH (incidence, onset, duration, and severity, associated symptoms like neck spasm and vomiting, methods of treatment).
Each patient was visited 6, 24, 36, 48 and 72 hours postoperatively to check for the presence or absence of PDPH, its onset and severity. Severity of headache was graded as per Lybecker classification [6].
Any patient with dural puncture was included even if she/he experienced a surgical complications (bleeding, injury, hysterectomy), failed spinal, total spinal, or even request to have general anaesthesia after the spinal.
Patients diagnosed as having PDPH were not discharged till they became symptom free. Patients were advised to take bed-rest, avoid straining and were given additional fluids and analgesics in the form of NSAIDS, paracetamol as required.
Statistical Analysis
The results in the study are presented in a tabulated manner as mean ± Standard Deviation (SD). Data was statistically analysed using SPSS (Version 23.0). For categorical data, Chi-Square test, for numerical data for inter group comparison, one way analysis of variance (ANOVA) test and Z test was applied for comparison of proportion between two groups. P-value ofless 0.05 was considered statistically significant.
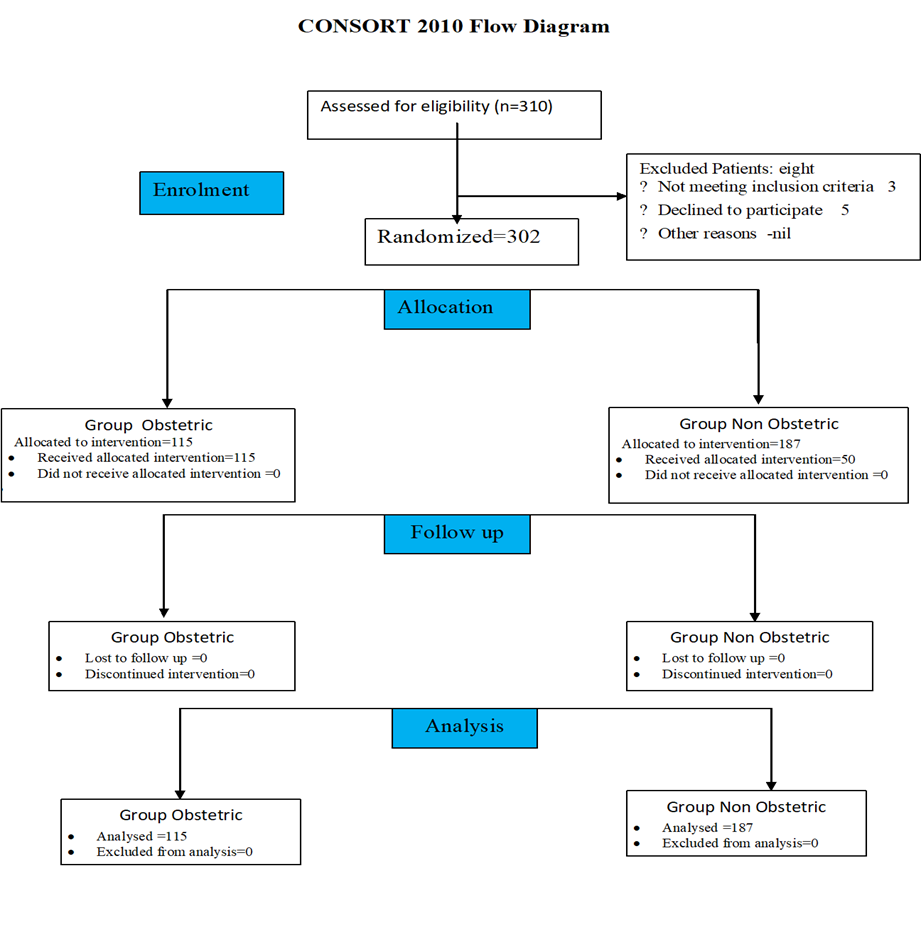
Figure 1: Flow Chart of Patients Recruited and Analyzed in Two Groups
Table 1: Demographic Profile of the Patients in Two Groups
Variables
Parameters
Group Obstetric (n= 115)
Group Non Obstetric (n=187)
p-value
Age (yrs)*
20-30
92 (80%)
55 (29.3%)
0.0001
31-40
23 (20.0%)
31 (16.6%)
>40
0 (0.0%)
101 (54.0%)
Mean±SD
30.66± 6.27
52.88±12.72
0.045
BMI (Kg /m2)*
Mean±SD
23.01 ±1.4
22.90 ±1.3
0.529
Gender
(Female/male) † (Number)
115/0
76/111
0.001
ASA Status
(Number/%)
I†
0(0.0%)
142(75.9%)
0.001
II
115(100.0%)
45(24.1%)
Note: Data expressed as* mean±SD and †number as appropriate. BMI: Body Mass Index, ASA: American Society ofAnaesthesiologist’s physical status.
Table 2: Methods of Management of Pdph in the Patients
Variable (Methods of Management)
Number/% of patients
Fluid and bed rest
5(29%)
Fluid +bed rest+acetaminophen
6(35.2%)
Fluid +bed rest+acetaminophen+NSAIDs
6(35.2%)
Epidural blood patch
-
Observations and Results
The present observational study was carried out to evaluate the method of Management, Complications and Patient satisfaction among obstetrics and non-obstetrics and undergoing surgeries under subarachnoid block were enrolled comprising of parturients as well, over a period of 18 months at the Department of Anaesthesia, Dr RPGMC Kangra at Tanda. The five patients were excluded due to unwillingness to participate in the study and three patients couldn’t meet inclusion criteria. Thereby 302 patients were randomized into 2 groups. The total patients included were 302, being 115 in obstetric group and 187 in non-obstetric group (Figure 1).
Table 3: Association of Duration of Pdph and Type of Patients in Two Groups
Variable
Obstetric
Non-obstetric
p-value
Duration of the PDPH
Day 1
2(25%)
-
0.056
Day 2
5(62.5%)
4(44.4%)
Day 3
1(12.5%)
4(44.4%)
Day 4
1(11.1%)
patients having Post Dural Puncture Headache (PDPH) after undergoing surgeries under subarachnoid block in a Tertiary Care Hospital. A total of 310 patients aged 20-60 years belonging to ASA I, II having BMI less than 30 kg/m2
Table 4: Incidence of Nausea and Vomiting in Two Groups
Nausea and vomiting
Obstetric n=111
Non obstetric group n=187
p-value
Yes
10(8.7%)
14(7.5%)
0.8743
No
105(91.3%)
173(92.5%)
Table 5: Associated Complication in the Two Groups in Perioperative Period
Any other complication
Obstetric n=111
Non-Obstetric n=187
p-value
Blurred vision
0(0.0%)
1(0.53%)
0.972
Low backache
0(0.0%)
1(0.53%)
Vertigo
3 (2.61%)
3 (1.6%)
No
112 (97.39%)
182 (97.3%)
Table 6: Patient Satisfaction In Two Groups
Patient satisfaction
Obstetric n=111
Non-Obstetric n=187
p-value
Satisfied VAS>5
62(53.9%)
80(42.8%)
0.0778
Very Satisfied VAS>7
53(46.1%)
107(57.2%)
Mean age of patients in group obstetric and group non obstetric was 30.66± 6.27 years and 52.88±12.72 years respectively (P=0.045). In our study, majority of obstetric population aged between 20-30 years, while 54% of non-obstetric population was aged above 40 years (P Value=0.0001) (Table-1).
Mean BMI of patients in group obstetric and group non obstetric was 23.01±1.4 kg/m2 and 22.90±1.3 kg/m2 respectively (P=0.529). With regards to gender distribution in the non-obstetric group, 76 were female patients, while 111 were male (P Value=0.001). In relation to ASA grading 145 patients belonged to ASA I in non-obstetric group, whereas 42 patients belonged to ASA II in non-obstetric group and 115 in obstetric group (P Value=0.001) (Table-1).
In our study, 29% of the patient responded to the fluid and bed rest, whereas 35.2% patients required acetaminophen tablet as well, however 35.2% patients required the non-steroidal anti-inflammatory drugs as well. No patient in either group required epidural blood patch.
All patients with PDPH had resolution of their symptoms by conservative management (hydration, bed rest, acetaminophen and NSAIDS), the PDPH resolved in 2(25%) of the parturients within the 1st day of its commencement. Whereas 5 parturients (62.5%) and 4 patients (44.4%) in non-obstetric group had relief on 2ndday after commencement of the headache. One parturient (12.5%) and 4 patients (44.4%) in non-obstetric group got relief on the 3rd day. One patient in non-obstetric group (11.1%) had relief on the fourth day.
In obstetrics and non-obstetrics population, incidence of nausea and vomiting was in 8.7% and 7.5% patients respectively.
In obstetrics and non-obstetrics population, other complications were in 2.61% and 2.7% subjects respectively.
In obstetrics and non-obstetrics population, patient satisfaction was comparable (P=0.0778). None of the patients in our study complained of severe PDPH and no patient required interventional treatment like epidural blood patch.
DISCUSSION
Spinal block is a reliable and easy technique frequently used in the anaesthetic practice. The post dural puncture headache (PDPH) is a well-known complication of spinal block.7 The PDPH, which cause significant morbidity in obstetric patients, has higher incidence because of the increased cerebrospinal fluid (CSF) pressure related to pregnancy, dehydration, blood loss, postpartum diuresis, hormonal imbalance, high serum estrogen levels, and increased peridural pressure [8-9].
In our study, the incidence of post dural puncture headache was 7% in parturients and 4.8% in non-obstetric patients (P=0.597). Whereas in the study by Srivastava et al. [10] the incidence was 4% in the obstetric group as compared to none in non-obstetric group(P=0.045) with 27 G quincke spinal needle. The lesser incidence in this study could be attributed to 27 G needle. Whereas in the study by Makito et al. [11] the incidence was 0.16% and 1.16% in the obstetric and non-obstetric patients respectively.Moreover, on the contrary the study by Weinrich J et al. [12] observed that the incidence of PDPH was less in obstetric patients (1.8%) as compared to orthopaedic patients(5.9%). The more incidence in orthopaedic patients may be because of delayed ambulation in such patients as compared to obstetric patients. In study by DelPizzo K et al. [13] 3.4% of patients for ambulatory lower limb surgery developed PDPH after subarachnoid block with 27 G pencil point spinal needle.
In most of the studies [11-15], Immediate exacerbation in symptoms and radicular pain are described and these symptoms don’t persist and relieve with administering simple pain killers and other supportive measures like rehydration, acetaminophen, NSAID’s and antiemetic therapy. Long term complications are less. Similarly in our study all patients with PDPH had resolution of their symptoms by conservative management (hydration, bed rest, acetaminophen and NSAIDS). Similarly, in our study, in obstetrics and non-obstetrics population, incidence of nausea and vomiting was in 8.7% and 7.5% patients respectively and other complications were in 2.61% and 2.7% subjects respectively.
CONCLUSION
The present study concluded that obstetric population had higher incidence of PDPH in comparison to non-obstetric population. All patients with PDPH had resolution of their symptoms by conservative management (hydration, bed rest, acetaminophen and NSAIDS) within 3-4 days while incidence of nausea and vomiting and other complications like backache, vertigo were very less.
REFERENCE
Gogarten, W. and Aken, V.H. "A century of regional analgesia in obstetrics." *Anesth Analg*, vol. 91, no. 1, 2000, pp. 773–775.
Michie, A.R. *et al.* "Subarachnoid anaesthesia for elective caesarean section." *Anaesth*, vol. 43, no. 1, 1988, pp. 96–99.
Arnold, M. "Headache classification committee of the international headache society the international classification of headache disorders." *Cephalalgia*, vol. 38, no. 1, 2018, pp. 1–21.
Cesur, M. *et al.* "Decreased incidence of headache after unintentional dural puncture in patients with caesarean delivery administered with postoperative epidural analgesia." *J Anesth*, vol. 23, no. 1, 2009, pp. 31–35.
Oedit, R. *et al.* "Efficacy of the epidural blood patch for the treatment of post lumbar puncture headache BLOPP: a randomised, observer-blind, controlled clinical trial." *BMC Neurol*, vol. 5, no. 1, 2005, pp. 12–17.
Castrillo, A. *et al.* "Postdural puncture headache: impact of needle type. a randomized trial." *Spine J*, vol. 15, no. 1, 2015, pp. 1571–1576.
Kiki, I. *et al.* "A simple, safe and effective approach to prevent postdural puncture headache: epidural saline injection." *European J Med*, vol. 41, no. 1, 2009, pp. 175–179.
Bezov, D. *et al.* "Post-dural puncture headache: part I diagnosis, epidemiology, etiology, and pathophysiology." *Headache*, vol. 50, no. 1, 2010, pp. 1144–1152.
Srivastava, V. *et al.* "Study of post dural puncture headache with 27g quincke & whitacre needles in obstetrics / non obstetrics patients." *MEJ Anesth*, vol. 20, no. 1, 2010, pp. 711–717.
Makito, K. *et al.* "Incidences and risk factors for post-dural puncture headache after neuraxial anaesthesia: a national inpatient database study in Japan." *Anesth Intensive Care*, vol. 48, no. 1, 2020, pp. 381–388.
Weinrich, J. *et al.* "Postdural puncture headache after neuraxial anesthesia: incidence and the risk factors." *Der Anaesthesist*, vol. 69, no. 1, 2020, pp. 878–885.
DelPizzo, K. *et al.* "Risk of postdural puncture headache in adolescents and adults." *Anesth Analg*, vol. 131, no. 1, 2020, pp. 273–279.
Uluer, M.S. *et al.* "A randomized study to evaluate post-dural puncture headache after caesarean section: comparison with median and paramedian approaches." *Niger J Clin Pract*, vol. 22, no. 1, 2019, pp. 1564–1569.
Hirachan, N. "Incidence of post dural puncture headache in parturients following early ambulation and recumbency." *Journal of Patan Academy of Health Sciences*, vol. 4, no. 1, 2017, pp. 14–20.
Advertisement
Recommended Articles
Research Article
Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India
Rahul Rai,
...
Tushar
Published: 05/04/2025
Download PDF
Cite
x
APA
Rai, R., Paul, D. & None, T. (2025). Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India. Himalayan Journal of Medicine and Surgery, 6(1), 1-3.
MLA
Rai, Rahul, Dharam Paul and Tushar . "Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India." Himalayan Journal of Medicine and Surgery 6.1 (2025): 1-3.
Chicago
Rai, Rahul, Dharam Paul and Tushar . "Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India." Himalayan Journal of Medicine and Surgery 6, no. 1 (2025): 1-3.
Harvard
Rai, R., Paul, D. and None, T. (2025) 'Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India' Himalayan Journal of Medicine and Surgery 6(1), pp. 1-3.
Vancouver
Rai R, Paul D, Tushar T. Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India. Himalayan Journal of Medicine and Surgery. 2025 Jan;6(1):1-3.
Download PDF
Review Article
Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review
Dharam Pau,
Tushar
Published: 05/04/2025
Download PDF
Cite
x
APA
Pau, D. & None, T. (2025). Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review. Himalayan Journal of Medicine and Surgery, 6(1), 1-3.
MLA
Pau, Dharam and Tushar . "Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review." Himalayan Journal of Medicine and Surgery 6.1 (2025): 1-3.
Chicago
Pau, Dharam and Tushar . "Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review." Himalayan Journal of Medicine and Surgery 6, no. 1 (2025): 1-3.
Harvard
Pau, D. and None, T. (2025) 'Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review' Himalayan Journal of Medicine and Surgery 6(1), pp. 1-3.
Vancouver
Pau D, Tushar T. Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review. Himalayan Journal of Medicine and Surgery. 2025 Jan;6(1):1-3.
Download PDF
Research Article
Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra
Shallabh Sharma,
Ashish Guleria
Published: 05/04/2025
Download PDF
Cite
x
APA
Sharma, S. & Guleria, A. (2024). Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra. Himalayan Journal of Medicine and Surgery, 5(1), 1-5.
MLA
Sharma, Shallabh and Ashish Guleria. "Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-5.
Chicago
Sharma, Shallabh and Ashish Guleria. "Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-5.
Harvard
Sharma, S. and Guleria, A. (2024) 'Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-5.
Vancouver
Sharma S, Guleria A. Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-5.
Download PDF
Research Article
A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla
Shivali Ranote,
...
Ashutosh
Published: 05/04/2025
Download PDF
Cite
x
APA
Ranote, S., Sharma, A. & None, A. (2024). A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla. Himalayan Journal of Medicine and Surgery, 5(1), 1-6.
MLA
Ranote, Shivali, Ajay Sharma and Ashutosh . "A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-6.
Chicago
Ranote, Shivali, Ajay Sharma and Ashutosh . "A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-6.
Harvard
Ranote, S., Sharma, A. and None, A. (2024) 'A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-6.
Vancouver
Ranote S, Sharma A, Ashutosh A. A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-6.
Negi, C., None, P. & Ram, M. (2022). Method of Management, Complications and Patient Satisfaction Among Obstetrics and Non-Obstetrics Patients Having Post Dural Puncture Headache (Pdph) After Undergoing Surgeries Under Subarachnoid Block in a Tertiary Care Hospital. Himalayan Journal of Medicine and Surgery, 3(2), 1-5.
MLA
Negi, C.M., Poonam and Mast Ram. "Method of Management, Complications and Patient Satisfaction Among Obstetrics and Non-Obstetrics Patients Having Post Dural Puncture Headache (Pdph) After Undergoing Surgeries Under Subarachnoid Block in a Tertiary Care Hospital." Himalayan Journal of Medicine and Surgery 3.2 (2022): 1-5.
Chicago
Negi, C.M., Poonam and Mast Ram. "Method of Management, Complications and Patient Satisfaction Among Obstetrics and Non-Obstetrics Patients Having Post Dural Puncture Headache (Pdph) After Undergoing Surgeries Under Subarachnoid Block in a Tertiary Care Hospital." Himalayan Journal of Medicine and Surgery 3, no. 2 (2022): 1-5.
Harvard
Negi, C., None, P. and Ram, M. (2022) 'Method of Management, Complications and Patient Satisfaction Among Obstetrics and Non-Obstetrics Patients Having Post Dural Puncture Headache (Pdph) After Undergoing Surgeries Under Subarachnoid Block in a Tertiary Care Hospital' Himalayan Journal of Medicine and Surgery 3(2), pp. 1-5.
Vancouver
Negi C, Poonam P, Ram M. Method of Management, Complications and Patient Satisfaction Among Obstetrics and Non-Obstetrics Patients Having Post Dural Puncture Headache (Pdph) After Undergoing Surgeries Under Subarachnoid Block in a Tertiary Care Hospital. Himalayan Journal of Medicine and Surgery. 2022 Jul;3(2):1-5.