Caecal volvulus is the axial rotation of the ascending colon, cecum, and terminal ileum. It was first described by Rokitansky in 1837 [4]. Caecal volvulus could be divided into two major groups of loop axial ileocolic, the commonest, accounting for 90% of cases, which can appear as a clockwise or counter clockwise pattern in which the latter one is the most commonly seen variety [3]. Caecal bascule is where there is an upward folding of the cecum either anteriorly or posteriorly [5].
Caecal volvulus is said to be associated with inadequate right colon fixation or anomalies in which the right colon does not properly fuse to the lateral peritoneum [6]. Other well documented predisposing factors for CV are long-standing constipation, distal obstruction, previous abdominal surgeries, intraabdominal masses, being bedridden, and undergoing colonoscopy procedures [5,7].When it occurs in the younger populations its more commonly caused by post-OP adhesions, pregnancy, or aganganglionic megacolon [7-9] Reports have shown that there is no sex predilection and the mean age of incidence is 61.8 years6 .
The clinical presentation depends on the duration of the complaints and the presence of complications. Symptoms of abdominal pain, associated with vomiting and abdominal distension, are reported as the commonest presentations [5]. Preoperative diagnosis of CV poses a significant challenge because of its rarity and nonspecific symptoms, mostly diagnosed intraoperatively.We were also able to reach the diagnosis intraoperatively [10]. Laboratory investigations are neither specific nor sensitive for the diagnosis of CV but may suggest the degree of obstruction and presence of complications [11].
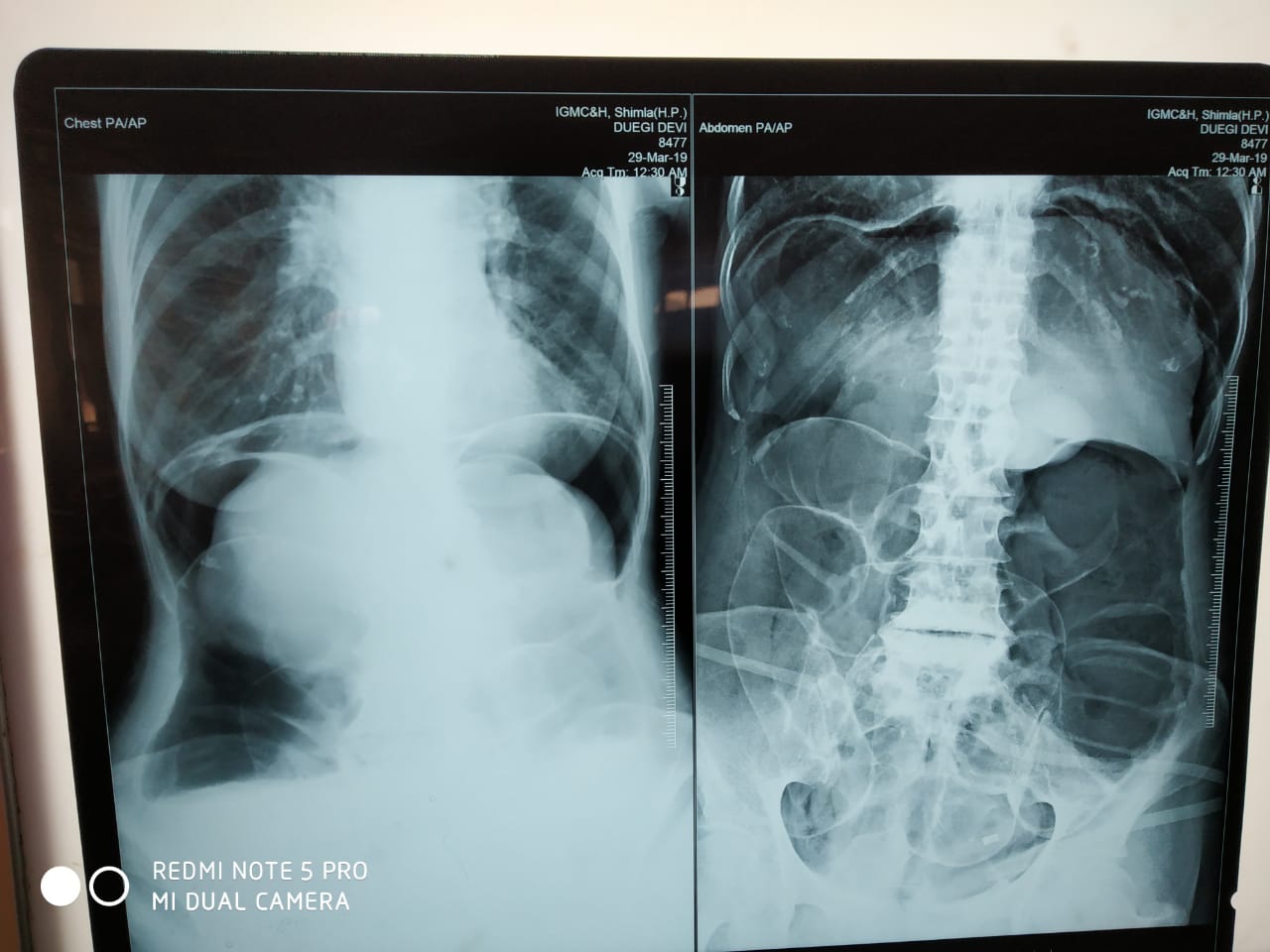
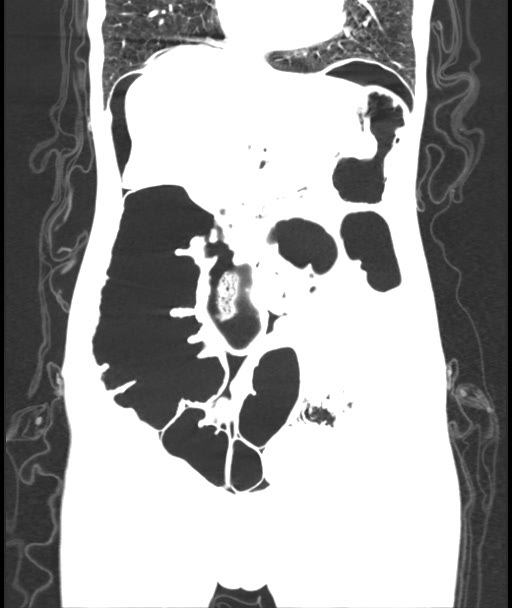
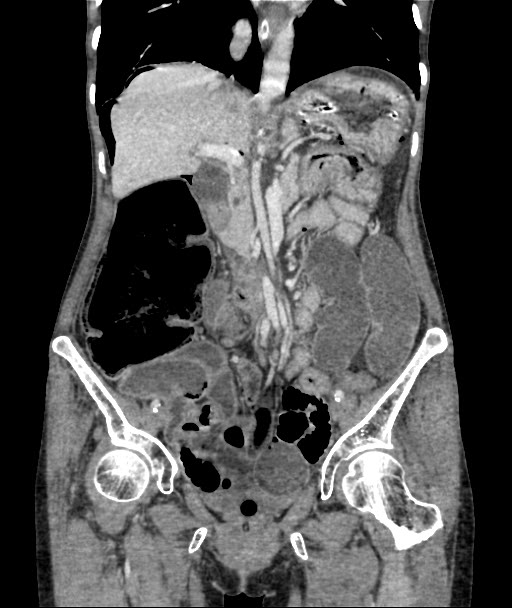
Radiologic imaging may be abnormal and detect CV in 45–56% of the cases [5] .Plain abdominal x-ray is highly sensitive for the diagnosis of CV with the characteristic “coffee bean“ sign deformity, its apex pointing to the left upper quadrant [9]. Other findings commonly seen are cecal dilatation (98−100%), single air–fluid level (72–88%), small bowel dilatation (42–55%), and absence of gas in the distal colon (82%). CT is more sensitive and specific for diagnosing CV and detecting complications [10].
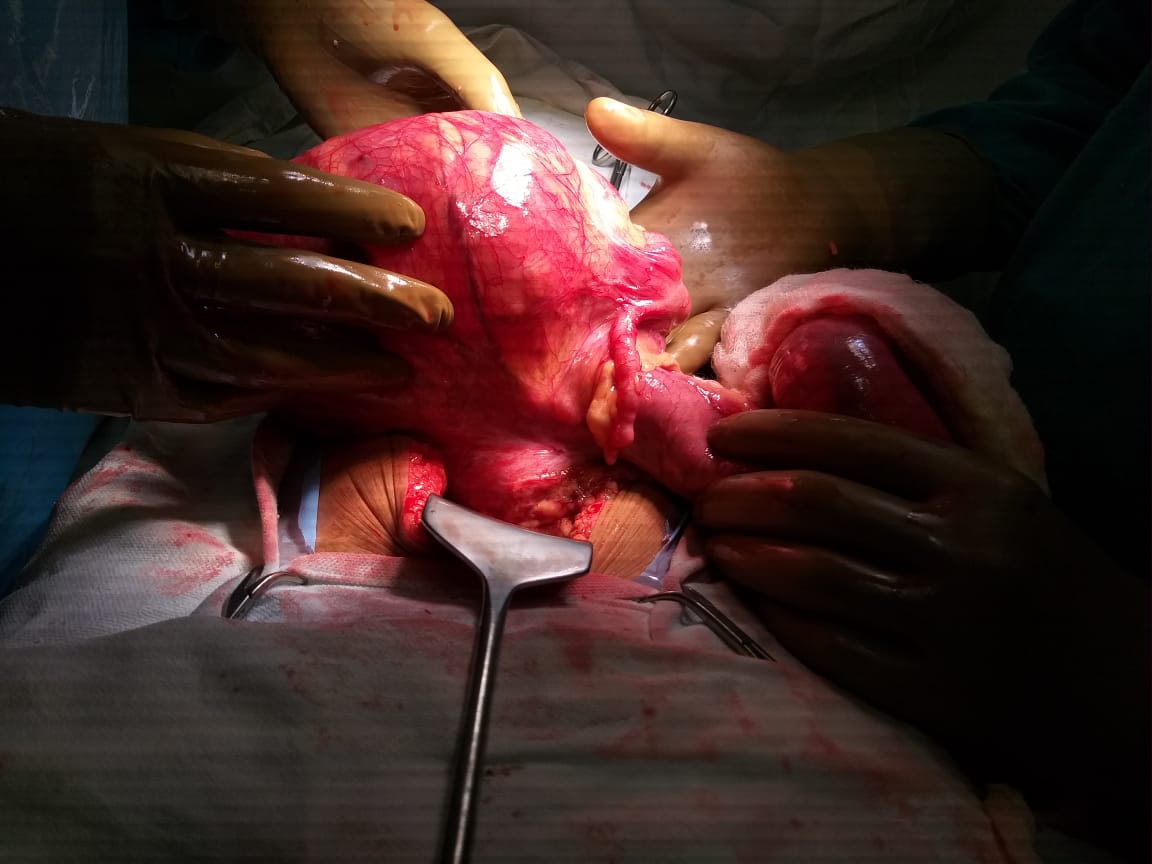
Once the diagnosis of CV was made patients should undergo urgent laparotomy or laparoscopic procedures to untwist the segment early to avoid the risk of strangulatio [5].
Once exploration has been done and if the intraoperative finding is a volvulated cecum; its viability should be assessed. Resection (right hemicolectomy) for all gangrenous and perforated or grossly distended thinned out cecal volvulus is the treatment of choice with primary anastomosis, ileostomy with mucous fistula is depending on the patient’s intraoperative physiology and bowel condition, resection has the absolute advantage of eliminating the risk of recurrence [5].
Manual detorsion without resection options is not advisable since it is associated with an unacceptable risk of recurrence (40%) [6]. Cecopexy or cecostomy are also available options depending on the overall status of the patient. Possible endoscopic detorsion in cecal volvulus is an emerging option for non-strangulated volvulus but associated with high risk of recurrence [12].