Objectives: Previous study shows that’s females with PCOS have higher ratio of LH/FSH ratio than those healthy females. Although this ratio is not so sensitive but its help in the diagnosis of PCOS. The ophthalmological effect of high LH/FSH ratio have yet not been investigated in women with PCOS. The aim of current study to compare the corneal thickness (CCT) of patients with PCOS and those healthy women. Methods: A case control study of 111 women were included in this study,69 of the were PCOS and 42 age and gender matched health women were in rolled in this study. CCT was measured for both PCOS and healthy women by tachymetry. LH, FSH and LH/FSH ratio measured for PCOS individuals. Results: Women with high ratio PCOS shows no significant changes in CCT in Comparison with normal ratio PCOS women. Also women with high ratio PCOS shows no significant changes in CCT in Comparison to healthy individuals. So, no significant correlation between LH, FSH hormone levels and CCT. Conclusion: Although the PCOS has target organ effects on the eye, consequently it's seems no direct effect on CCT. We suggest a careful and detail corneal evaluation in PCOS patients to prevent the potential risk of CCT changes in addition to already known complications.
Keywords
Polycystic Ovarian Syndrome (PCOS)
Corneal Thickness (CCT)
LH
FSH Hormone Levels
INTRODUCTION
The Cornea
In the simplest terms, the cornea is a fibre-reinforced fluid membrane, which its tensile strength derived from the three-dimensional organization of collagen fibers and its bulk properties derive from the inter febrile fluid pressure [1]. The cornea lacks the neurobiological [1] sophistication of the retina and the dynamic movement of the lens; yet, without its clarity, connective tissue that acts as the primary infectious and structural barrier of the eye infections [2].
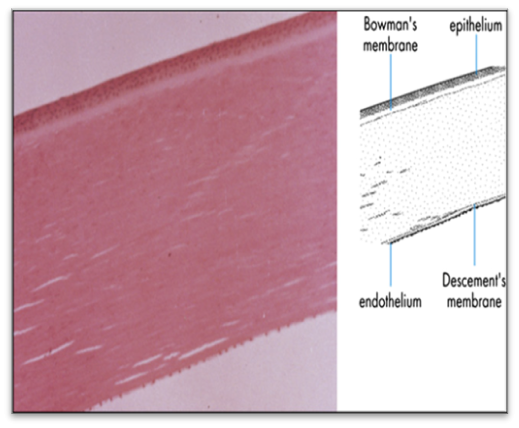
The cornea has five principal layers which, from anterior to posterior, are the epithelium, Bowman’s, stromal, Descemet’s and endothelium. Bowman’s and Descemet’s layers are basement membranes for the cellular epithelium and endothelium layers, respectively. The stromal occupies 90% of the cornea’s thickness and like other soft, highly hydrated and charged collagenous tissues such as cartilage and intervertebral disc, is a polyelectrolyte gel consisting of a mixture of interacting fluid, solid and ionic phases. Water is the principal component of stromal which saturates the collagen solid phase solvates the ionic phase and accounts for about 78% of the cornea by weight [3].
In the average adult, the horizontal diameter of the cornea is 11.5 to 12.0 mm and about 1.0 mm larger than the vertical diameter. It is approximately 0.5 mm thick at the center and gradually increases in thickness toward the periphery. The shape of the cornea is prorated flatter in the periphery and steeper centrally which creates an aspheric optical system [4].
Figure 1: Light micrograph of normal endothelium (original magnification_100). Note the single-cell endothelial layer with a Descemet membrane of uniform thickness (epithelial surface at top of figure). Reprinted with permission of Ophthalmology.4 Copyright 2008Elsevier
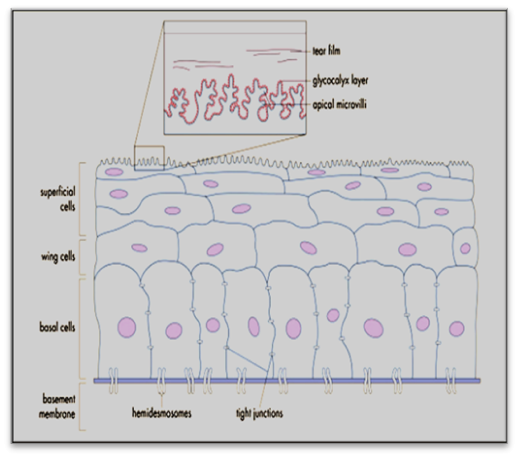
Figure 2: Cross-sectional view of the corneal epithelial cell layer Reprinted with permission of Ophthalmology.4 Copyright 2008 Elsevier
Corneal shape and curvature are governed by the intrinsic biomechanical structure and extrinsic environment. Anterior corneal stromal rigidity appears to be particularly important in maintaining the corneal curvature. Organizational differences in the collagen bundles of the anterior stromal may contribute to a tighter cohesive strength in this area and may also explain why the anterior curvature resists change to stromal hydration much more than the posterior stromal, which tends to more easily develop folds . Stromal hydration also appears to affect the cornea’s response to strain and shear forces.
The human cornea consists of 5 recognized layers, 3 cellular (epithelium, stromal, endothelium) and 2 inter- face (Bowman membrane, Descemet membrane [5] (Fig - 1).
Epithelium
The epithelial surface of the cornea creates the first barrier to the outside environment and is an integral part of the tear film–cornea interface that is critical to the refractive power of the eye. Embryo logically, the corneal epithelium is derived from surface ectoderm between 5 and 6 weeks of gestation. It is composed of no keratinized, stratified squamous epithelium that is 4 to 6 cell layers thick (40 mm to 50 mm) [6].
The mucinous layer of the tear film, which is in direct contact with the corneal epithelium, is produced by the conjunctiva goblet cells and interacts closely with the corneal epithelial cell glycocalyx to allow hydrophilic spreading of the tear film with each eyelid blink.
Anatomy of the Cornea
The life span of corneal epithelium is ten days, which regularly undergoes apoptosis (programmed cell death) [7].
The tear film prohibit from interring the intercellular spaces by tight junction between neighbors surface cells.
Basal layer is the deep cellular layer which composed of single cell layer which the only cell layer cab able of mitosis(stem cells).They are source of wing cells [8].
0.05Mm is the epithelium basement membrane thickness, once it is injured needs 4-6 weeks to heals, during this period the epithelial attachment is tends to be weak.
Bowman Layer
Its 15Mm thickness, help to maintain corneal shape once its injured can't regenerates and replaced by scar tissue.
Stroma
It provides 80-85% of the corneal thickness, it differs from other collagenous structures by its transparency due to highly arrange collagens fibers and extracellular matrix [9-10].
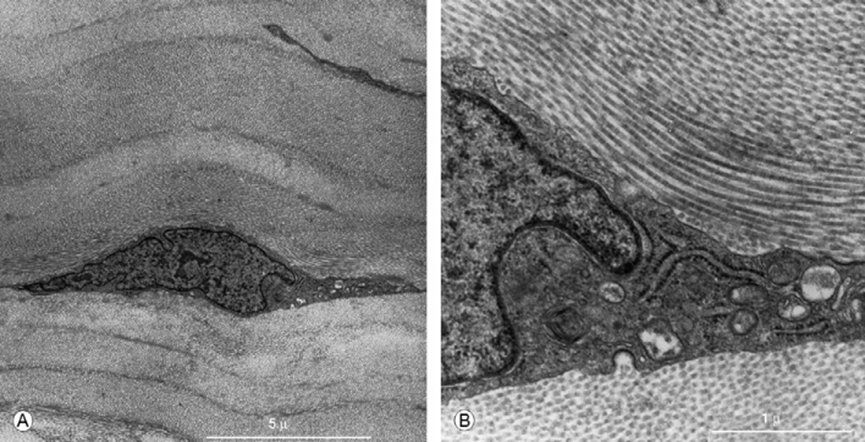
Figure 3: Transmission electron microscopy of the human corneal stromal. A Keratocyte localized between stromal lamellae B: Higher magnification view. Showing a keratocyte in relation to collagen fibers coursing in various directions Reprinted with permission of Cornea.6 Copyright 2005 Elsevier
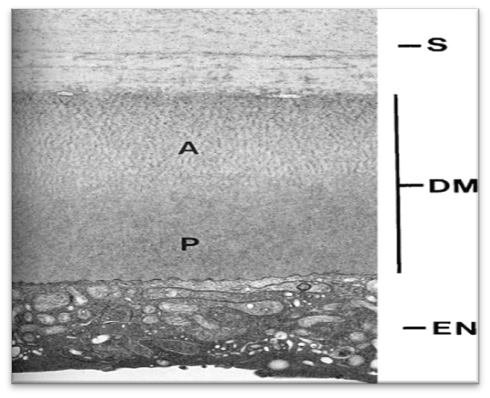
Figure 4: Micrograph illustrating Descemet membrane (DM) located between the posterior aspect of the corneal stromal (S) and the underlyin endothelium (EN). The anterior “banded” region (A) is secreted by the endothelial cells during fetal development and is more highly organized than the posterior “amorphous region” region” (P), which is secreted after birth. Reprinted with permission of Principles and Practice of Ophthalmology. [13] Copyright 2008 Elsevier
An additional feature of the stromal is that the ultrastructure within the organization of the lamella appears to vary based on the depth within the stromal.
Deeper layers are more strictly organized than superficial layers, and this difference accounts for the greater ease of surgical dissection in a particular planes one approaches the posterior depths of the corneal stromal. This variation in stromal organization also accounts for the differences in response to corneal edema, as mentioned previously.
Descemet folds are the result of asymmetric swelling of the posterior stromal imposed by the structurally more rigid anterior cornea and structural restriction imposed by the limbs.
Stromal swelling is therefore directed posteriorly and results in relative flattening of the posterior surface, which can push Descemet membrane into multiple folds that become visible as striate [11-12].
Keratocytes are the major cell type of the stromal and are involved in maintaining the ECM environment. They are able to synthesize collagen molecules and glycosaminoglycans while also creating matrix metalloproteases (MMPs) dall crucial in maintaining stromal homeostasis.
Descement Membrane
At 8 weeks of gestation the endothelial cells start to secret it continuously The anterior 3 mm secreted prior to birth has a distinctive banded appearance when viewed by electron microscopy, but Descemet membrane produced after birth is unbranded and has an amorphous ultra-structural texture. Descemet can accumulate up to 10 mm in thickness with age (Figure 4).
Endothelium
The endothelium act on maintaining corneal clarity by keeping it relatively deturgesced state. It`s monolayer with honey comb mosaic from posterior view [14].
It`s 15Mm in thickness which span the posterior portion of the entire cornea and fused with trabecular [15]. The lateral membranes contain a high density of NaC, KC-ATPase pump sites [16].
The basal surface of the endothelium contains numerous hemi desmosomes that promote adhesion to Descemet membrane. Endothelial cell density and topography continue to change throughout life. From the second to eighth decades of life, the cell density declines from 3000to 4000 cells/mm2 to around 2600 cells/mm2, and the percentage of hexagonal cells declines from approximately 75% to approximately 60% [17].
Blood Supply of the Cornea
The cornea is avascular tissue 'where it met it`s need from blood components, through a tiny blood vessels at the limbs, tear film and aqueous humor.
Nerve Supply of the Cornea
The most sensitive and heavily innervated tissue in the body is the cornea, which derived from nasocillary branch, branch of ophthalmic nerve.
Overview of Gonadotropins
The gonadotropins, a family of closely related glycoprotein hormones includes the followings: follicular stimulatory hormone (FSH), luteinizing hormone (LH) which is secreted by same pituitary cells; gonadotropins and chorionic gonad tin (CG) which placental origin.
Gonadotropin-releasing hormone (GnRH) is adecapeptide secreted from the pre-optic and arcuate nuclei of the hypothalamus into the hypophyseal-portal blood vessels which transports it to the anterior pituitary. At anterior pituitary GnRH stimulates the secretion of LH and FSH, both of which play a central role in ovarian function [19].
The key hormone regulating follicular growth is FSH, while pulsatile LH appears to be involved in regulating normal follicular turnover. Our knowledge of the chemistry of the gonadotropic hormones has greatly increased our understanding of the mechanisms of mammalian reproduction. LH and FSH are synthesized in the pituitary gland, released into the systemic blood circulation, and carried to the target end organs the gonads where the production of (20) androgens and estradiol's.
In the ovary, the cellular contribution to steroid genesis is very different from that in the testis, and both granulose cells and theca cells contribute to steroid genesis. In the test is supporting cell lineage gives rise to Sterol cells which are nurse cells for spermatogenesis. For ovarian histogenesis, the supporting cell lineage gives rise to granulose cells. Theca cells develop from stromal steroid genic precursor cells outside the follicles and are ovarian counterparts of lending cells. The theca cells synthesize androgen in response to human chorionic gonadotropin, hCG and pituitary LH [21].
Polycystic Ovarian Syndrome
Definition and Diagnostic Criteria
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in women and major cause of an-ovulatory infertility.
The diagnosis based on thee ESRHE/ASRM Rotterdam consensus meeting in 2003, which broaden the previous NIH criteria classifications of1991 [22].
At least two out of these criteria 2003 Rotterdam criteria:
Oligo-or anovulation
Clinical and or biochemical signs of hyperandrogenism
Echogenic evidence of polycystic ovaries and exclusion of other causes of hyperandrogenism and anovulation [23]
Etiology
The Etiology of Pcos Is Unknown
It is theorized that early exposure to androgen excess in utero or during neonatal, period is associated with development of the PCOS phenotype later in life [24-27]
Genetic basis is associated with several candidate genes for insulin resistance and androgen production (eg,cytochrome p450c17,cytochrome p450c11a,and insulin receptor substrate)
Central obesity play direct role in pathophysiology of PCOS by contributing to insulin resistance and increase androgen level
A high percentage (55-75 %) of women with PCOS have an elevated LH/FSH ratio presumably due to high levels of LH rather than reduced production of FSH. GnRH stimulation causes, indeed, excessive LH production [28] in those women. This condition may be determined by a higher frequency or amplitude of GnRH [29] it is not yet clear whether alteration of the hypothalamo-pituitary axis in PCOS is primary or secondary to alterations in steroid hormones secretion. The role of FSH is to recruit ovarian follicles and stimulate their growth: 2-5 mm follicle are sensitive to FSH whereas larger ones (6-8 mm) acquire aromatase activity and may increase estradiol (E2) and inhibit B reducing levels of FSH in late follicular stage. On the other hand, PCOS patients (having LH and FSH concentrations higher and lower than normal, respectively).
Clinical Features
The three distinguishing features include:
Hyperandrogenism: clinical sign include hirsutism acne and hair loss [30]
Chronic anovulation: fewer than eight episodes per a year [31]
Ultrasonographic evidence of polycystic ovaries: The polycystic ovary was defined as having≥10 follicles (2–8 mm), anovarian volume≥12 cm3, and a bright echogenic stromal [32]
Luteiizing Hormone/Follicle Stimulating Hormone (Lh/Fsh) Ratio
A ratio>2.0 is suggestive of PCOS but it`s not highly sensitive.
Gonadotropin levels are affected by oral contraceptives [33].
Hirsutism
Define as excessive hair loss of suggests under lying hyperandrogensim it`s frequently seen on the upper lip, chest, back, chin and lower abdomen [34].
Other criteria are hyperinsulinemia, elevated insulin like factor (IGF_1), obesity.
MATERIALS AND METHODS
Patients and Methods
A case control study for 111 woman done in the ophthalmology department of AL SADDER MEDICAL CITY for the period from December 2015 to September 2016. Women included in this study were any women in her reproductive age attending the outpatient department in our hospital in Dermatology Department which has been already diagnosed as PCOS and sent for laser therapy for hirsuitism (IPL). Questionnaire for each patient include age, marital state, no. of children, address, any medical and surgical history, drug history and hormonal therapy and any eye surgery.
Their investigation was reviewed for hormonal levels and U/S criterion for PCOS.
The control group are relatives of the patients and any female that have negative history for polycystic ovary, normal hormonal assay and nomal U/S.
Exclusion Criteria
Patients with any corneal and ocular surface pathology, his- tory of eye surgery, ocular trauma, any topical medications patients with systemic diseases: DM, hypertension systemic drugs (amiodaron), metabolic disorder like cystinosis.
Patients with other endocrinopathies, pituitary adenoma, Hyperprolactinemia, pregnant ladies were also excluded.
Endocrinological Assessment
Includes hormonal level measurement of both LH and FSH hormones at day 3 and 4 from the menstrual cycle measured in IU for patients with PCOS in the lab of the infertility center.
LH/FSH ratio were calculated, resulted in normal ratio PCOS and high ratio PCOS patients.
Ophthalmological Assessment
Patients underwent corneal examination by slit lamp bio microscopy in ophthalmological department of AL-SADDER MEDICAL CITY for both control and PCO patients group
Measurements of CCT by pentagm (pachymetry) for Rt and Lt corneas for both control and disease groups expressed in Mm
Statistical analysis
Statistical analysis was done by using SPSS (statistical package for social sciences) version 20 in which we use independent sample t-test and pearson correlation coefficient for numerical data and chi square with odds ratio for categorical data. P value≤0.05 regarded significant.
RESULTS
A total of 111 women had been included in this study. Twenty nine of them had PCO with normal LH: FSH
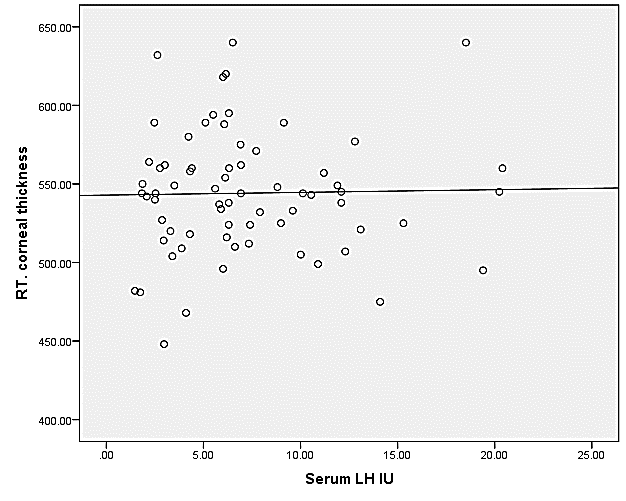
Figure 5: Correlation between serum LH level and right corneal thickness
Note: r=-0.013 p=0.782
ratio (group 1), 40 had high LH:FSH ratio (group 2) and 42 control group (group 3).
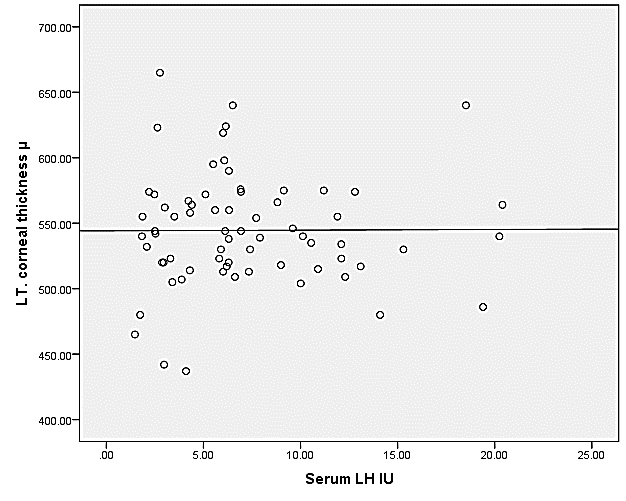
Figure 6: Correlation between serum LH level and left corneal thickness
Note: r=-0.035 p=0.545
Table 1: Demographic characteristics of women under study
Marital status
Groups
p value
Normal ratio (n=29)
High ratio (n=40)
Control (n=42)
Married
25(86.2%)
32(80%)
32(76.2%)
0.581
Unmarried
4(13.8%)
8(20%
10(23.8%)
Age/years
29.551±8.862
31.225±7.287
31.904±6.539
0.422
Table 2: Comparison between group 1 and 3 in corneal thickness
Groups
RT. Cornea
LT. cornea
p value
Normal ratio (n=29)
541.4483±38.17683
33.50206±45.40619
0.656
Control (n=42)
537.6190±33.50206
538.8095±34.33709
0.563
Note: Values are expressed in mean ± SD. P>0.05
Table 3: Association between PCO (normal ratio) and corneal thickness(right)
Groups
RT cornea
Total
OR (95%CI)
<=546
>546
Normal ratio
15
14
29
0.659
(0.253-1.719)
51.7%
48.3%
100.0%
Control
26
16
42
61.9%
38.1%
100.0%
Total
41
30
71
57.7%
42.3%
100.0%
There is no significant association between right corneal thickness and PCO (normal ratio)
Table 4: Association between PCO (normal ratio) and corneal thickness (left)
Groups
LT cornea
Total
OR (95%CI)
<=546
>546
Normal ratio
15
14
29
0.659
(0.253-1.719)
51.7%
48.3%
100.0%
Control
26
16
42
61.9%
38.1%
100.0%
Total
41
30
71
57.7%
42.3%
100.0%
There is no significant association between left corneal thickness and PCO (normal ratio)
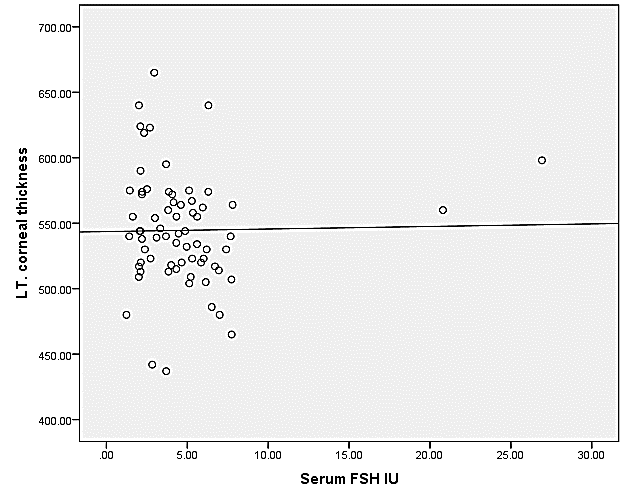
Figure 7: Correlation between serum FSH level and left corneal thickness
Note: r=-0.036 p=0.823
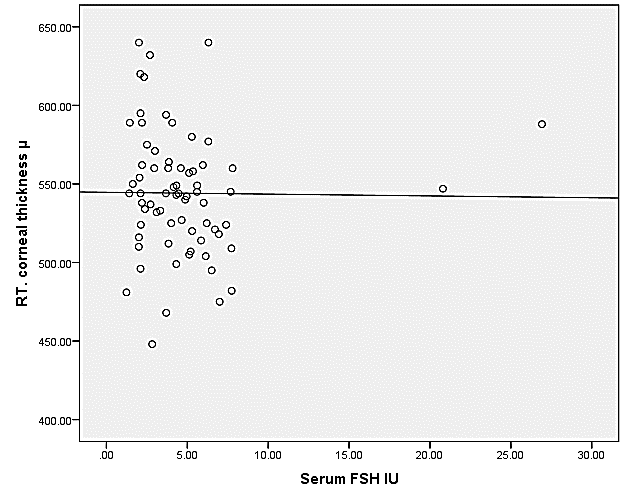
Figure 8: correlation between serum FSH level and right corneal thickness
Note: 0.014 p=0.785
Table 5: Comparison between group 2 and 3 in corneal thickness.
Groups
RT. cornea
LT. cornea
p value
High ratio (n=40)
546.0750±40.53
544.7250±41.82073
0.305
Control (n=42)
537.6190±33.5
538.8095±34.33
0.485
Values are expressed in mean ± SD. P>0.05
Table 6: Association between PCO (high ratio) and corneal thickness (right)
Groups
RT cornea
Total
OR (95%CI)
<=546
>546
High ratio
24
16
40
0.923 (0.38-2.24)
60.0%
40.0%
100.0%
Control
26
16
42
61.9%
38.1%
100.0%
Total
50
32
82
61.0%
39.0%
100.0%
There is no significant association between high ratio group and right corneal thickness
Table 7: Association between PCO (high ratio) and corneal thickness (left)
Groups
LT cornea
Total
p value
<=546
>546
High ratio
25
15
40
1.026 (0.42-2.505
62.5%
37.5%
100.0%
Control
26
16
42
61.9%
38.1%
100.0%
Total
51
31
82
62.2%
37.8%
100.0%
There is no significant association between high ratio group and left corneal thickness
Table 5 shows no significant difference in cornea between group 2 and 3.
Figure 5 shows no significant correlation between serum LH and right corneal thickness.
Figure 6 shows no significant correlation between serum LH and left corneal thickness.
Figure 7 shows no significant correlation between serum FSH and left corneal thickness.
Figure 8 shows no significant correlation between serum FSH and right corneal thickness.
DISCUSSION
Polycystic ovarian syndrome (PCOS) is the most common gynecological endocrinopathy [58].
PCOS appears to be associated with an increased risk of metabolic aberrations, including insulin resistance and hyperinsulinism, type 2 diabetes mellitus, dyslipidemia, cardiovascular disease, and endometrial carcinoma [59].
A total of 111 women had been included in this study. Twenty nine of them had PCO with normal LH:FSH ratio (group 1), 40 had high LH:FSH ratio (group 2) and 42 control group (group 3).
Demographic data of studied group 1:
Demographic characteristics of women under study. Table 1 shows no significant difference between groups regarding age and marital status (P value=0.581,0.422 respectively).
Results in Table 2 show Comparison between group 1 (Patients with PCO and normal:
LH\FSH ratio) and group3 (control group) in CCT for the right cornea for each group according to study in Lithuanian population for CCT (546±13) [78] The CCT was (541.44±38.17), (537.61±33.50) and for left cornea, (544.3103±45.40619), (538.8095±34.33709) where no significant diffirence between these two groups where p value±(0.656,0.563) respectively.
This result disagree to one recent report,corneal thickness in patients with PCO was found to be higher than amoung controls:this finding attributed to higher IGF-1 levels in patients with PCO [60].
It has been suggested that this association may give rise to more serious eye diseases such as glaucoma [61].
Table 3 association between PCO with normal ratio and right CCT.
Results shows no significant associations in Rt CCT between control and PCO (normal ratio) ,51.7% are ≤546 and 38.5% >546.as OR=0.569.
Table 4 Association between PCO (normal ratio) and Rt CCT.Theres no significant association between, Rt CCT and PCO were 51.7%≤546 and 48.3% > 546, OR=0.659.
Figure 1,2 correlation of serum LH level and Rt and Lt CCT (Group 1).
Shows no significant correlation between serum level and CCT as (r=0.137) (p=0.476).
The result shows no significant correlation between serum LH and Rt CCT. In group one this result is disagree with previous study result where they found patient with PCO had higher level of CCT in Comparison with control patient they suggest this might attributed to high levels IGF-1 which found to be higher in those patients as the cornea is possible target [61-62].
While many women with PCOS still have LH and FSH still within the 5-20 mlU/ml range, their LH level is often two or three times that of the FSH level. For example, it is typical for within the normal range of 5-20 mlU/ml). This situation is called an elevated LH to FSH ratio or a ratio of 3:1 so there is no real elevation in LH hormone in PCO patients rather than elevated ratio which might help in diagnosis [63].
Figure (3)(4) correlation between FSH level and Rt and Lt CCT. In this figure there is no significant correlation, (r=0.13 p=0.5) and (r=0.129 p=0.506).
As this due to the fact that the hormonal level of PCO remain within the normal levels for both LH and FSH. For most of the patients if we compare our result with study of normal pregnant females how shows increase in CCT versus normal non pregnant females.
As pregnant female show little changes in FSH level as the pregnancy proceed [64].
This changes in corneal thickness causes by corneal oedema as apart of the generalized oedema occurs in pregnants ladies especially in final trimester which is statistically significant only in the31-40 wk (p=0.01) [65-66]
Table 5 Comparison between group 2 and group 3 in CCT, which shows no significant difference. P=0.305, 0.485 respectively.
Table 6 association of CCT in group 2, i.e high ratio, for RT and left cornea.
Results in no significant association for both Rt and left cornea, percentage of CCT >546 is 40%,37% FOR Rt and Lf eye respectively.
This result is inconsistent with other studies for CCT in PCO as there is significant increase in the corneal thickness [62].
In the other hands other study also show significant increase in CCT and tear film instability in patients with PCO [61].
To compare our study with other study for evolution of corneal thickness during menstrual cycle which shows a significant increase in CCT for both eyes during preovulatry and ovulatory time which coincide with LH surge, their result shows increase CCT at days 1 and 3 was 541.40+-11.36 and 540.80±11.70 microne for Rt and Lf cornea respectively.
Corneal thickness was not stastically different in Rt and Lt eyes at any time (p<0.05) [67].
These changes could be secondary to hormonal influences; estrogen receptors can be found in human corneas, suggesting that estrogen may have a role in corneal physiology; [69]. Another study demonstrated that there is a significant change in corneal hydration during the normal menstrual cycle. Apparently, the change is associated with the effects of estrogen more than with progesterone. The authors believe one might assume ready access of these hormones via the aqueous humor or tear film because of their high lipid solubility. They suggest that another possibility would be an indirect action of hormones on the cornea via their effects on tear film osmolarity [68].
CONCLUSION
There is no direct correlation between the CCT and LH/FSH ratio, this might be attributed to small studied group, we might need large sample size
As the results are non-significant, it might be belongs to the fact that there is no increase in hormonal level and remain in normal range, but there is only increase in the ratio
Recommendations
Further studies and increase sample size might be needed to assess the effects of LH/FSH on CCT
Enquiry about the hormonal therapy for induction of ovulation may affect CCT
Timing of menstrual cycle and the time of the measurement of CCT, should be take in account
pregnant ladies have higher readings so should be excluded from the study
Any topical and systemic hormonal therapy may affect the result, so should put in the mind
Cautions should be taken in account for patients with PCO when they ask about LASIK surgery
REFERENCE
Elliott, G. F. and S. A. Hodson. “Cornea, and the swelling of polyelectrolyte gels of biological interest.” 1998.
Maurice, D. M. “Clinical physiology of the cornea.” J Cataract and Refractive Surgery, vol. 37, no. 4, 2011, pp. 588–598.
Rüfer, F. et al. “White-to-white corneal diameter; normal values in healthy humans obtained with the Orbscan II topography system.” Cornea, vol. 24, no. 3, 2005, pp. 259–261.
Muller, L. J et al. “The specific architecture of the anterior stromal accounts for maintenance of corneal curvature.” British Journal of Ophthalmology, vol. 85, no. 4, 2001, pp. 437–443.
Farjo, A et al. “Corneal anatomy, physiology, and wound healing.” Ophthalmology, edited by M. Yanoff and J. S. Duker, 3rd ed., Mosby, 2008, pp. 203–208.
Hanna, C., Bicknell, D. S. and J. E. O’Brien. “Cell turnover in the adult human eye.” Archives of Ophthalmology, vol. 65, 1961, pp. 695–698.
Wiley, L. et al. “Regional heterogeneity in human corneal and limbal epithelia: an immunohistochemical evaluation.” Investigative Ophthalmology and Visual Science, vol. 32, no. 3, 1991, pp. 594–602. http://www.iovs.org/content/32/3 /594.full.pdf.
Li, W. et al. “Niche regulation of corneal epithelial stem cells at the limbus.” Cell Research, vol. 17, no. 1, 2007, pp. 26–36. http://www.nature.com/cr/journal/v17/n1/pdf/7310137a.pdf.
Boote, C. et al. “Collagen fibrils appear more closely packed in the prepupillary cornea: optical and biomechanical implications.” Investigative Ophthalmology and Visual Science, vol. 44, no. 7, 2003, pp. 2941–2948. http://www. iovs.org/content/44/7/2941.full.pdf.
Gipson, I. K. and N. C. Joyce. “Anatomy and cell biology of the cornea, superficial limbus, and conjunctiva.” Principles and Practice of Ophthalmology, edited by D. M. Albert and F. A. Jakobiec, 3rd ed., Saunders, 2008, pp. 423–420.
Fini, M. E. and B. M. Stramer. “How the cornea heals; cornea-specific mechanisms affecting surgical outcomes.” Cornea, vol. 24, suppl. 1, 2005, pp. S2–S1.
Beebe, D. C. and J. M. Coats. “The lens organizes the anterior segment: specification of neural crest cell differentiation in the avian eye.” Developmental Biology, vol. 220, 2000, pp. 424–431.
Watsky, M. A et al. “In vitro corneal endothelial permeability in rabbit and human: the effects of age, cataract surgery and diabetes.” Experimental Eye Research, vol. 49, 1989.
Stiemke, M. M et al. “The developing corneal endothelium: correlation of morphology, hydration and Na/K ATPase pump site density.” Current Eye Research, vol. 10, 1991.
Yee, R. W. et al. “Changes in the normal corneal endothelial cellular pattern as a function of age.” Current Eye Research, vol. 4, 1985, pp. 671–678.
Oliveira-Soto, L. and N. Efron. “Morphology of corneal nerves using confocal microscopy.” Cornea, vol. 20, 2001, pp. 374–384.
Mullen, M. P et al. 2013.
Childress, D. and J. R. Gingrich. 2010.
Sevin, G., et al. “Androgens and anabolic steroids.” 2008.
Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. “Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS).” Human Reproduction, vol. 19, 2004, p. 417.
Franks, S et al. “Development of polycystic ovary syndrome: involvement of genetic and environmental factors.” International Journal of Andrology, vol. 29, 2006, pp. 278–285.
De Leo, V et al. “Insulin-lowering agents in the management of polycystic ovary syndrome.” Endocrine Reviews, vol. 24, 2003, pp. 633–667.
Homburg, R. et al. “The relationship of serum anti-Müllerian hormone with polycystic ovarian morphology and polycystic ovary syndrome: a prospective cohort study.” Human Reproduction, vol. 28, 2013, p. 1077.
Abbott, D. H et al. “Developmental origin of polycystic ovary syndrome-a hypothesis.” Journal of Endocrinology, vol. 174, 2002, p. 15.
Kalro, B. N et al. “Neuromodulation in polycystic ovary syndrome.” Obstetrics and Gynecology Clinics of North America, vol. 28, 2001, pp. 35–36.
Thomson, R. L et al. “Vitamin D in the aetiology and management of polycystic ovary syndrome.” Clinical Endocrinology, vol. 77, 2012, pp. 343–350.
Azziz, R. et al. “Position statement: criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society Guideline.” Journal of Clinical Endocrinology and Metabolism, vol. 91, no. 11, 2006, pp. 4237–4245.
Norman, R. J. et al. “Polycystic ovary syndrome.” Lancet, vol. 370, no. 9588, 2007, pp. 685–697.
Amer, S. A. et al. “An evaluation of the inter-observer and intra-observer variability of the ultrasound diagnosis of polycystic ovaries.” Human Reproduction, vol. 17, no. 6, 2002, pp. 1616–1622.
Banaszewska, B. et al. “Division of Infertility and Reproductive Endocrinology.” Poznan University of Medical Sciences, vol. 48, 2003.
Rosenfield, R. L. “Clinical practice: hirsutism.” New England Journal of Medicine, vol. 353, no. 24, 2005, pp. 2578–2588.
Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. “Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome.” Fertility and Sterility.
Tsai, C.-P. et al. “Corneal lesions as the initial manifestation of tyrosinemia type II.” Journal of the Chinese Medical Association, vol. 69, 2006, pp. 286–288.
El-Abassi, R., Singhal, D. and J. D. England. “Fabry’s disease.” Journal of the Neurological Sciences, vol. 344, 2014, pp. 5–19.
Shovlin, J. P. “Corneal manifestations of systemic disease.” Review of Optometry, Jan–Feb 2005, pp. 30–33.
Tsai, C-P., et al. “Corneal lesions as the initial manifestation of tyrosinemia type II.” Journal of the Chinese Medical Association, vol. 69, 2006, pp. 286–288. http://dx.doi.org /10.1016/S1726-4901(09)70259-X.
El-Abassi, R., et al. “Fabry’s disease.” Journal of the Neurological Sciences, vol. 344, 2014, pp. 5–19. http://dx. doi.org/10.1016/j.jns.2014.06.
Shovlin, J. P. “Corneal manifestations of systemic disease.” Review of Optometry (Review of Corneal and Contact Lenses Supplement), Jan. /Feb. 2005, pp. 30–33.
Gahl, W. A., et al. “Corneal crystals in nephropathic cystinosis: Natural history and treatment with cysteamine eye drops.” Molecular Genetics and Metabolism, vol. 71, 2000, pp. 100–120. http://dx.doi.org/10.1006/mgme. 2000 .3062.
Buchan, B., et al. “Gel formulations for treatment of the ophthalmic complications in cystinosis.” International Journal of Pharmaceutics, vol. 392, 2010, pp. 192–197. http://dx.doi.org/10.1016/j.ijpharm.2010.03.065.
Fenu, M., et al. “Kayser-Fleischer ring in Wilson’s disease, a cohort study.” European Journal of Internal Medicine, vol. 23, 2012, pp. e150–e156. http://dx.doi.org/10.1016/j.ejim. 2012.04.005.
Mc Cluskey, P. and R. Powell. “The eye in systemic inflammatory disease.” The Lancet, vol. 364, 2004, pp. 2125–2133. http://dx.doi.org/10.1016/S0140-6736(04)1 7554-5.
Robbins, S. L., et al. Pathologic basis of disease. 3rd ed., WB Saunders, 1984, pp. 1356–1362.
Kunimoto, S. M., et al., editors. Cornea. In: Wills eye manual: Office and emergency room diagnosis and treatment of eye disease, 4th ed., Lippincott Williams and Wilkins, 2004, e-book.
Nguyen, C. Q. and A. B. Peck. “Unraveling the pathophysiology of Sjögren syndrome associated dry eye disease.” The Ocular Surface, vol. 7, 2009, pp. 11–27. http://dx.doi.org/10.1016/S1542-0124 (12)70289-6.
Hamideh, F. and P. E. Prete. “Ophthalmologic manifestations of rheumatic disease.” Seminars in Arthritis and Rheumatism, vol. 30, 2001, pp. 217–241. http://dx.doi.org/ 10.1053/sarh.2001.16639.
Driebe, W. T. and S. S. Bhatia. “Superior limbic keratoconjunctivitis.” In: Krachmer, J. H., et al., editors. Cornea, 2nd ed., Elsevier Mosby, 2005, pp. 713–718.
T. E., et al. “Endocrine and metabolic differences among phenotypic expressions of polycystic ovary syndrome according to the 2003 Rotterdam consensus criteria.” American Journal of Obstetrics & Gynecology, vol. 198, 2008, pp. 670.e1–670.e1.
Legro, R. S. “Polycystic ovary syndrome and cardiovascular disease: A premature association?” Endocrine Reviews, vol. 24, 2003, pp. 302–312. doi:10.1210/er.2003-0004.
Kebapcilar, A. G., et al. “Cornea in PCO.
Bonni, S., et al. “Itchy dry eye associated with polycystic ovary syndrome.” American Journal of Ophthalmology, vol. 143, 2007, pp. 763–771.
Kebapcilar, A. G., et al. Archives of Gynecology and Obstetrics, 2014.
Best-Boss, Angela and Evelina Weidman Sterling. Living with PCO, with Richard Legro.
Hirano, M., et al. “Department of Obstetrics and Gynecology, Tohoku University School of Medicine.” Tohoku Journal of Experimental Medicine, vol. 118, 1976, pp. 275–282.
British Journal of Ophthalmology, vol. 61, 1977, pp. 646–649.
Ghahfarokhi, Negar Amiri, et al., 2015.
Leach NH et al. "Corneal hydration during the menstrual cycles." [Journal name missing], 1971.
Giuffrè G et al. "Variations in central corneal thickness during the menstrual cycle in women." [Journal name missing], vol. 26, 2007, pp. 144–146, Lippincott Williams and Wilkins, Inc.
Leach NE et al. "Corneal hydration changes during the normal menstrual cycle: a preliminary study." Journal of Reproductive Medicine, vol. 6, 1971, p. 2014.
Katz B et al. "Recurrent crystal deposition after keratoplasty in nephropathic cystinosis." American Journal of Ophthalmology, vol. 104, 1987, p. 190.
Sher NA et al. "The ocular manifestations in Fabry's disease." Archives of Ophthalmology, vol. 97, 1979, p. 671. Ellis PP. "Ocular deposition of copper in hypercupremia." American Journal of Ophthalmology, vol. 68, 1969, p. 423.
Ellis PP. "Ocular deposition of copper in hypercupremia." American Journal of Ophthalmology, vol. 68, 1969, p. 423.
Smith RE and Schanzlin DJ. "Rheumatoid diseases." In: Smolin G and Thoft RA, eds. The Cornea: Scientific Foundations and Clinical Practice, 3rd ed., Little Brown, 1994, p. 364.
Collier M. "La pathologie cornéènne des diabétiques." Bulletin de la Société d'Ophtalmologie de France, vol. 67, 1967, p. 105.
Foulks GN et al. "Factors related to corneal epithelial complications after closed vitrectomy in diabetics." Archives of Ophthalmology, vol. 97, 1979, p. 1076.
Foster CS and Yee M. "Corneoscleral manifestations of Graves' disease, the acquired connective tissue disorders, and systemic vasculitis." International Ophthalmology Clinics, vol. 23, 1983, p. 131.
Coksuer H et al. "Effect of hyperandrogenism on tear function and tear drainage in patients with polycystic ovary syndrome." Journal of Reproductive Medicine, vol. 56, 2011, pp. 65–70.
Galgauskas S et al. "Age-related changes in corneal thickness and endothelial characteristics." Clinical Interventions in Aging, 2014.
None
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Medicine and Surgery open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Recommended Articles
Research Article
Phenotypic Characterization and Antimicrobial Resistance Patterns of Clinical Klebsiella pneumoniae Isolates from Al-Najaf Teaching Hospital
Anfal Abdulhussain Jawad,
Hind AL-Hammami
Published: 30/06/2026
Download PDF
Cite
x
APA
Abdulhussain Jawad, A. & AL-Hammami, H. (2026). Phenotypic Characterization and Antimicrobial Resistance Patterns of Clinical Klebsiella pneumoniae Isolates from Al-Najaf Teaching Hospital. Himalayan Journal of Medicine and Surgery, 7(1), 1-6.
MLA
Abdulhussain Jawad, Anfal and Hind AL-Hammami. "Phenotypic Characterization and Antimicrobial Resistance Patterns of Clinical Klebsiella pneumoniae Isolates from Al-Najaf Teaching Hospital." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-6.
Chicago
Abdulhussain Jawad, Anfal and Hind AL-Hammami. "Phenotypic Characterization and Antimicrobial Resistance Patterns of Clinical Klebsiella pneumoniae Isolates from Al-Najaf Teaching Hospital." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-6.
Harvard
Abdulhussain Jawad, A. and AL-Hammami, H. (2026) 'Phenotypic Characterization and Antimicrobial Resistance Patterns of Clinical Klebsiella pneumoniae Isolates from Al-Najaf Teaching Hospital' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-6.
Vancouver
Abdulhussain Jawad A, AL-Hammami H. Phenotypic Characterization and Antimicrobial Resistance Patterns of Clinical Klebsiella pneumoniae Isolates from Al-Najaf Teaching Hospital. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-6.
Download PDF
Research Article
Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori
Noor Zuhair Bakheet N. Z.
Published: 20/02/2026
Download PDF
Cite
x
APA
N. Z., N. Z. B. (2026). Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery, 7(1), 1-4.
MLA
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-4.
Chicago
N. Z., Noor Z. B.. "Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-4.
Harvard
N. Z., N. Z. B. (2026) 'Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-4.
Vancouver
N. Z. NZB. Impact of Gut-Liver Axis: Hepatic Biochemical and Metabolic Changes Associated with Chronic Gastritis in Iraqi Patients with Helicobacter Pylori. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-4.
Download PDF
Research Article
Effect of Land Degradation on Livelihood
Kemalo Abdulmalik,
Isreal Zewide
Published: 04/01/2024
Download PDF
Cite
x
APA
Abdulmalik, K. & Zewide, I. (2024). Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery, 5(1), 1-4.
MLA
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-4.
Chicago
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-4.
Harvard
Abdulmalik, K. and Zewide, I. (2024) 'Effect of Land Degradation on Livelihood' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-4.
Vancouver
Abdulmalik K, Zewide I. Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-4.
Download PDF
Research Article
Awareness and Practices among Professional Healthcare Workers towards COVID-19 in Iraq
Yasir H Motlaq,
...
Zainab T. N M. Almuhannah
Published: 30/03/2024
Download PDF
Cite
x
APA
H Motlaq, Y., A Aqebian, E. & N M. Almuhannah, Z. T. (2024). Awareness and Practices among Professional Healthcare Workers towards COVID-19 in Iraq. Himalayan Journal of Medicine and Surgery, 5(1), 1-9.
MLA
H Motlaq, Yasir, Esraa A Aqebian and Zainab T. N M. Almuhannah. "Awareness and Practices among Professional Healthcare Workers towards COVID-19 in Iraq." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-9.
Chicago
H Motlaq, Yasir, Esraa A Aqebian and Zainab T. N M. Almuhannah. "Awareness and Practices among Professional Healthcare Workers towards COVID-19 in Iraq." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-9.
Harvard
H Motlaq, Y., A Aqebian, E. and N M. Almuhannah, Z. T. (2024) 'Awareness and Practices among Professional Healthcare Workers towards COVID-19 in Iraq' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-9.
Vancouver
H Motlaq Y, A Aqebian E, N M. Almuhannah ZT. Awareness and Practices among Professional Healthcare Workers towards COVID-19 in Iraq. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-9.
Ali Khudhair Alamiry, N. & Kareem Ali Al-Dahan, A. (2023). The Effect of Gonadotropines Changes In Polycystic Ovarian Syndrom Patients on the Corneal Thickness. Himalayan Journal of Medicine and Surgery, 4(2), 1-9.
MLA
Ali Khudhair Alamiry, Najlaa and Ali Kareem Ali Al-Dahan. "The Effect of Gonadotropines Changes In Polycystic Ovarian Syndrom Patients on the Corneal Thickness." Himalayan Journal of Medicine and Surgery 4.2 (2023): 1-9.
Chicago
Ali Khudhair Alamiry, Najlaa and Ali Kareem Ali Al-Dahan. "The Effect of Gonadotropines Changes In Polycystic Ovarian Syndrom Patients on the Corneal Thickness." Himalayan Journal of Medicine and Surgery 4, no. 2 (2023): 1-9.
Harvard
Ali Khudhair Alamiry, N. and Kareem Ali Al-Dahan, A. (2023) 'The Effect of Gonadotropines Changes In Polycystic Ovarian Syndrom Patients on the Corneal Thickness' Himalayan Journal of Medicine and Surgery 4(2), pp. 1-9.
Vancouver
Ali Khudhair Alamiry N, Kareem Ali Al-Dahan A. The Effect of Gonadotropines Changes In Polycystic Ovarian Syndrom Patients on the Corneal Thickness. Himalayan Journal of Medicine and Surgery. 2023 Jul;4(2):1-9.