Exotropia is an outward divergence of the eyes. The concomitant exotropia (angle of deviation the same in all positions of gaze and regardless of which eye is fixing . Surgical correction is either by strengthening procedure (resection) or weakening procedure (Recession) . Patients and methods: In this retrospective cross sectional study ,we studied the surgical outcomes of 64 patients, who underwent primary correction for exotropia by a single surgeon .The records were taken from Ibsar center in AL-Najaf city. The patients records were analyzed for the following parameters: Gender ,age, type of exotropia as( constant, intermittent, alternate exotropia), associated refractive error as( myopia , hypermetropia ,myopia or hypermetropia with astigmatism),associated amblyopia ,exotropia with vertical deviation ,type of surgery. Postoperative follow up was done by a same surgeon , in 1st day,1st weak, 1st month ,and 6th month or more . Results: A total of 64 cases with concomitant exotropia who underwent surgical management were enrolled in this study. The age of the studied group ranged 2 –61 years with a median age of 14 years. Majority of the patients; 55 /64 represented (85.9%), were managed with RR surgery while the remaining 9 patients managed with BLR . Gender distribution were 37 females vs. 27 males among the studied group . The postoperative outcome of the studied group was assessed according to the postoperative alignment which revealed that 50 patients had good alignment giving a rate of 78.1% while only 14 cases had misalignment in a rate of 21.9%. Conclusions: The results of this study are encouraging and show satisfactory ocular alignment and comparable to other studies around the world. Factors such as age, gender, preoperative visual acuity were not significant factors for favorable surgical outcome. Strabismus surgery can help to preserve or restore the binocular vision. Aim of the study : To determine the results of surgery of exotropia in one center and the same surgeon. And to evaluate factors affecting outcome of surgical alignment.
Keywords
Exotropia
Amblyopia
Alignment
Age
Gender
And preoperative visual acuity
Important Note
Key findings:
The study of 64 patients undergoing surgical correction for exotropia showed a 78.1% success rate in achieving good ocular alignment. Factors such as age, gender, and preoperative visual acuity did not significantly affect surgical outcomes. The results suggest that strabismus surgery can effectively restore or preserve binocular vision in patients with exotropia.
What is known and what is new?
Exotropia is an outward deviation of the eyes that can be corrected surgically using either strengthening (resection) or weakening (recession) procedures. This study evaluates the surgical outcomes of 64 patients with concomitant exotropia who underwent primary correction by a single surgeon. It found a 78.1% success rate in achieving good ocular alignment, with factors such as age, gender, and preoperative visual acuity not significantly affecting outcomes. These results add to the existing knowledge by providing specific surgical outcome data from a single center and surgeon.
What is the implication, and what should change now?
Implication is the study's findings suggest that surgical correction for exotropia can be effective, with a high success rate in achieving good ocular alignment. Surgeons and healthcare providers should consider strabismus surgery as a viable option for patients with exotropia, as it can help preserve or restore binocular vision. Continued research and evaluation of surgical outcomes are important to improve treatment strategies and outcomes for patients with exotropia.
Introduction
1.1. Back ground and definitions:
At adulthood the Visual perception is ultimate. Offering that all the developmental processes according to it, have took place appropriately, both before and after child birth. Inclusive of anatomical and physiological processes.
According to our knowledge at least, the query of the beginning of squint was first approached (scientifically) in the 19th century. A few hypotheses have been suggested. For example:
Von Graefe (1854) thought that mechanistic factors creating squint.
Donders (1863) insisted that refractive errors may be the cause of squint through their hyperlinks with accommodation.
Duane (1869) suggested that the excess in vergence innervation was the cause of squint.
Worth (1915) recommended that once there is no fusion of the photos of the two eyes created strabismus, and that a (center of fusion) in the brain was involved in this condition.
Chavasse (1939) clarified squint as a final result of an excess in reflexogenic action.
In spite of that, none of these theories have been proven. The identical holds is that the cause or the end result of squint related to loss of binocular single vision(BSV).Theimprovement of normal (BSV) is prevented in absence of alignment whereas, without (BSV), the alignment of both eyes becomes unneeded [1].
Nowadays, theories on the cause of squint have advanced and two hypotheses have as a result developed: a (motor versus sensory) concept and a (peripheral versus central) hypothesis. The former principle suggested that squint may additionally have a (motor) or (sensory) origin, while the latter hypotheses suggests that squint may have a (central) or (peripheral) origin. The different varieties of squint are consequently classified relying on those (motor versus sensory) or (central versus peripheral) oppositions [1] .
Normally the visual axis reach the point of fixation as it comes from nodal point and the centre of the fovea. In cases of normal (BSV) the binocular responsive cells which are located in the visual cortex in addition to fusion reflex which are responsible for picture alignement as well as visual axes of the both eyes that cross at the point of fixation all of them are responsible for (BSV) [2].
when ocular alignment present with no any stimulant for fusion ,this is called Orthophoria which is uncommon condition.
when the fusion is blocked and both eyes have a tendency to deviate this is called Heterophoria (phoria) . Any person may have slight phoria but the prsence of fusion reflex will control it. (Esophoria) and (exophoria) are types of phorea as the former means the imbalance is inwared while the later means the imbalance is outwared [2]. An exodeviation is controlled by fusion under normal viewing conditions. An exophoria is detected when binocular vision is interrupted , as during an alternate cover test. Exophoria is fairly common , so that when the amplitudes of fusional convergence is adequate and there is a small angle of strabismus , her the exophoria is asymptomatic. Prolonged detailed visual work may bring about asthenopia. Breakdown of an exophoria to an exotropia may occur transiently during a serious illness or after ingestion of sedatives or alcohol. Treatment is usually not necessary unless an exophoria progresses to intermittent exotropia or it causes asthenopic symptoms [3]. Decompensating phoria occur When the imbalance can not be managed because there is inadequate fusion , this condition is accompanied by (asthenopia) and (diplopia) the former reffered to as symptoms of binocular discomfort while the latter reffered to as double vision [3] .
when the visual axes of both eyes will not intersect at the point of fixation here the deviation is manifist and the condition is called heterotropia (tropia) . When there is misalignement of the pictures that comes from both eyes or when there is supression of pictures from the deviating eye at visual cortex , diplopia will present.Some times there is defect in ordinary binocular fusion mechanisms dvelopment or when there is inequality of refraction of both which is called (anisometropia) as a result of oculomotor imbalance. Adulthood heterotropia occur when there is failure of fusion, that cause impairment of vision in one eye. Mechanical limition of the extraocular muscles or weakness, or some times nerve supply damage may cause squint. Latent or manifest squint are commonest form of Horizontal deviation. Hypertropia and hyperphoria are both upward deviation, the first one is upward displacement of one eye relative to the the opposite eye while the second is upward imbalance which is latent. Hypotropia and hypophoria these are downward displacement [3].
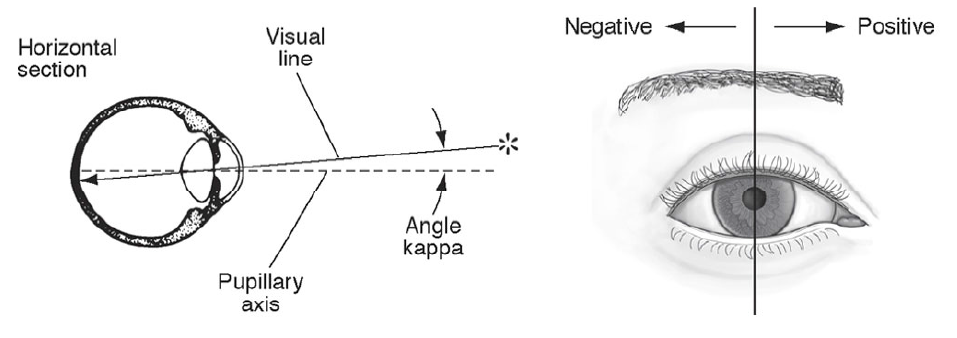
Anatomical axis is a line passing from the posterior pole through the centre of the cornea. Because the fovea lies in the anatomical centre at the posterior pole of the eye temporaly. The visual axes doesn't usually correspond to the anatomical axis of the eye (Figure1.1) (3). The angle between the anatomical and visual axes is called angle kappa it is usually about 5° . The corneal light reflex will be nasal to the centre of the cornea when the fovea is temporal to the pupillary axis, here the angle kappa is called positive angle kappa. exotropia will present when a positive angle kappa is large. While esotropia occure when the corneal light reflex is temporal to the center of the cornea and the fovia is nasal to the pupillary axis here the angle kapa is negative [3].
(Figure 1.1) Angle kappa. in case of exotropia (here the corneal light reflex is medial to the vertical line) angle kappa is positive, where as in esotropia (the light refex is lateral to the vertical line) angle kappa is negative [3].
1.2.Strabismus:is a condition in which there is loss of ocular alignment when looking at an object. This condition could be present occasionally or constantly. It may end in loss of depth perception or amblyopia If present in childhood period ,while diplopia may develop if present during adulthood. It may be due to ocular muscle defect , far sightedness , infection , trauma or any brain problems. Risk factors include , cerebral palsy , family history of the strabismus and premature birth are risk factors for the condition [3].
Patients and Methods
Study design and participants:
We analyzed medical records of 64 patients by reviewing them retrospectively; the patients had undergone surgical correction for concomitant exotropia by the same surgeon for a period from January 2012 to June 2019, at Ibsar Center in AL-Najaf city with a minimum postoperative follow-up of 6 months or more .The analyzed patients parameters were:
Patient’s age , it includes the following groups:
* ≤ 10 years (26 patients) .
*11 ـ20 years (16 patients) .
*21 ـ 30 years (15 patients) .
* > 30 years (7 patients) .
Patient’s gender:
* Female 37.
* male 27.
Cycloplegic refraction for young children.
Type of exotropia as constant, intermittent ,alternate exotropia .
Associated refractive error as myopia , hypermetropia ,myopia or hypermetropia with astigmatism .
Associated amblyopia .
Exotropia with vertical deviation .
Type of surgery.
Inclusion criteria are:
(1) all patients who were operated by the same surgeon.
(2) different age groups and both sexes.
(3) patients with 1st operation .
(4) all patients records that are available .
(5) patients who completed 6th month post operatively or more
exclusion criteria:
(1) if there was any prior strabismus surgery.
(2) presence of other significant ocular comorbidity (e.g. cataract, retinopathy of prematurity (ROP) treated with laser, optic nerve (ON) hypoplasia, etc. ).
(3) cerebral palsy, down syndrome or any other significant developmental delay.
(4) neurologic disorders such as epilepsy .
(5) loss of records.
(6) sensory squint .
(7) paralytic squint .
(8) A considerable alphabetic syndrome (‘A’ syndrome with more than 10 prism diopters deviation, or ‘V’ syndrome with greater than 15 prism diopters deviation between up and down gazes).
2.2. Preoperative examination :
All affected person had been examined preoperatively for
1. Best corrected visual acuity.
2. Squint’s angle before surgical treatment.
3. Amblyopia .
4.all patients underwent slit lamp bio microscopy and fundus examination.
5. Preoperative cycloplegic refraction; for patients younger than 5 years old, done with Atropine drop (IsoptoAtropine 0.5%) single drop two times daily at morning and evening for seven days. For patients who are older than 5 years, cycloplegic refraction done by Cyclopentolate drop ( Cyclogyl 0.5%) alternating with Tropicamide drop (Mydriacyl 1%), single drop into each eye every 5 minutes for 25 minutes.
Berens prism bar was used to measure the angle of deviation (far and near).
2.3.surgery:
The following surgical procedures were done under general anesthesia by asame surgeon:
1.Weakening procedures:
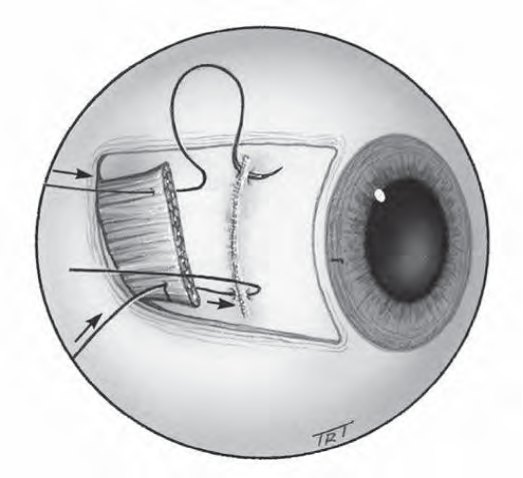
*Recession: is moving ocular muscle’s insertion away from its original insertion, this results in muscle weakening (slackening).
• Rectus muscle recession:
First the muscle is exposed, then the tendon of the muscle is disinserted after it’s being tied by two sutures (absorbable type) at its outer quarter. A caliper is used to measure the amount of the recession and mark it on the sclera, at last the dis inserted end of the muscle is sutured back to the sclera at the marked distance behind its original insertion .
(Figure 2.1)Recession of a horizontal rectus muscle. [4]
2.Strengthening procedures:
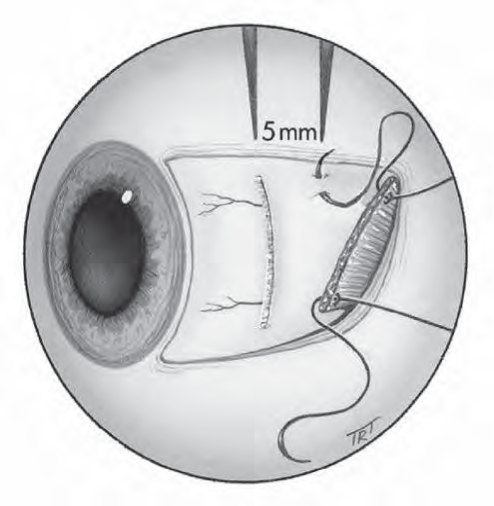
* Resection; is a procedure to strengthen the muscle effective pull by shortening it, this procedure is suitable only for recti.
It includes the following steps:
First the muscle is uncovered and a caliper is used to measure and mark resection distance; at the marked site two sutures of absorbable type are inserted. Then excision is done for the muscle anterior to the sutures, finally; the excised end is sutured back to the original insertion .
(Fig2.2) Resection of a horizontal rectus muscle. [4]
55 patients had the procedure done on one eye that is medial resection and lateral recession.
Combined lateral rectus recession in both eyes was done on 9 patient
Table (2.1) Surgical Amount for exodeviation.
Angle of exotropia,
BLRc
mm
BMRs
mm
MRs/LRc
mm
15
4.0
4.0
3.0/4.0
20
5.0
5.0
4.0/5.0
25
6.0
6.0
5.0/6.0
30
7.0
6.0/7.0
35
8.0
6.0/8.0
40
7.0+4.0
7.0/8.0
45
7.0+5.0
7.5/8.5
50
7.0+6.0
7.0/9.0
60
7.0
+5.0
8.0/10.0
70
7.0
+7.0
9.0/10.0
80
8.0
+7.0
10.0/10.0
BLRc :Bilateral Lateral rectus recession in millimeters
BLRs :Bilateral medial Rectus resection in millimeters
2.4.postoperative measurements:
Postoperative follow up was done by the surgeon ,in 1st day,,1stweak, 1stmonth,and 6th month and more .
Examination include:
1st day post operatively examination for alignment ,ocular motility and anterior and posterior segment examination.
1st weak postoperative included visual acuity , alignment and anterior segment examination for postoperative complication .
1stmonth and 6th month visual acuity ,alignment ,ocular motility.
The patients were grouped into good alignment and misalignment.
2.5.postoperative variables :
Postoperatively the patient may be in one of the following positions.
Unacceptable result:
1.residual exotropia: in which an angle of10 prism diopters (PD) or more is residual postoperatively.
2.large degree exotropia > 10 (PD) .
Good results:
Orthophoria ; perfect binocular alignment
Exotropia: (residual exotropia) less then 10PD.
2.6.ethical committee:
1.The study protocol was approved by theCouncil of Faculty of Medicine\ Kufa University and the department of ophthalmology .
2. patients identities were not disclosed during the study .
2.7.statistical analysis:
Using SPSS (the statistical package for social sciences) version 25, IBM, US; for managing and analyzing the data of the 64 patients. All data were checked for errors or inconsistency, using data cleaning methods. Descriptive statistics the variables presented as range, mean, median, standard deviation, inter quartile range (IQR), frequencies and percentage, according to the type of variable. Cross tabulation and chi square test used to assess the significance of relationship between postoperative alignment and other variables, including, age, gender, squint type, amblyopia, Type of surgery, presence of refractive errors and presence of vertical deviation. Student’s t test is used to compare the mean degree of deviation across the alignment status between the subgroups with misalignment and good alignment. Level of significance, P. value, set at ≤ 0.05, the value at which the difference or correlation is significant. Finally, results presented in tables and figures with an explanatory paragraph for each using the Microsoft Word and Excel Software, version 2013.
Results
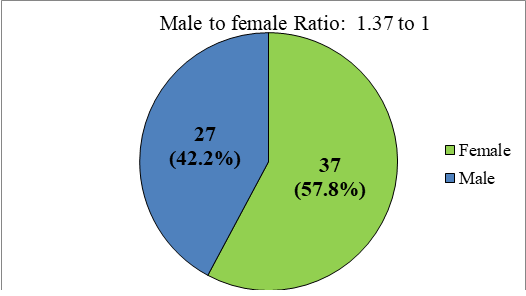
A total of 64 cases with concomitant exotropia who underwent surgical management were enrolled in this study. The age of the studied group ranged 2 – 61 years with a median age of 14 years, moreover, 40.6% of the cases aged 10 years or less, 25% aged 11 – 20 years, 23.4% aged 21 – 30 years and only 10.9% aged more than 30 years, indicated that majority of the cases, (89.1%), within the age of 30 years or less. Regarding the gender distribution, females were dominant, 37 ( 57.8%) females vs. 27 (42.2%) males among the studied group, with a female to male ratio of 1.37 to one, (Table 3.1 and Figure.3. 1).
For the Squint type, 25 patients (39.1%) had constant squint, 23 (35.9%) IE and 16 (25.0%) AE. On the other hand, Amblyopia was reported in 24 patients (37.5%), (Table 3.2).
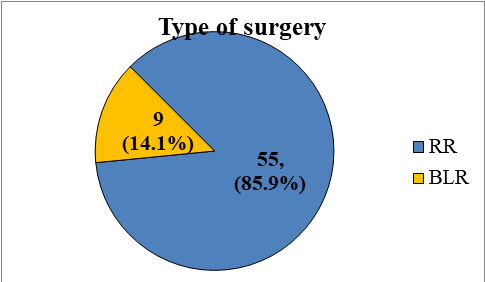
As it shown in (Figure3.2), majority of the patients; 55 /64 represented (85.9%), were managed with RR surgery while the remaining 9 patients managed with BLR.
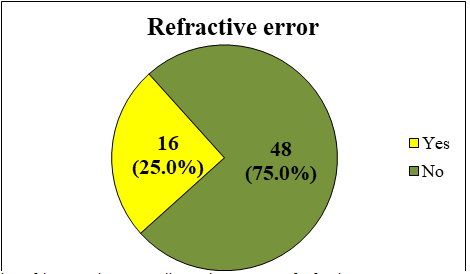
Refractive errors were documented in 16 patients, (25%), (Figure 3.3), these refractive errors as listed in (Table.3.3), out of these 16 cases, 7 (43.8%) with Myopia, 4 (25%) hypermetropia and 5 cases (31.2%) had Myopia or hypermetropia with astigmatism.
The frequency distribution of vertical deviation revealed that 10 cases (15.6%) had vertical deviation while 54 (84.4%) had not, on the other hand, the mean degree of deviation, was 35.8 ± 11.7 (range: 20 – 70) and a median of 35 with an interquartile range (IQR) of 30 – 40, this IQR indicated that more than 75% of the cases had a degree of deviation of 40 degree or less, (Table .3. 4).
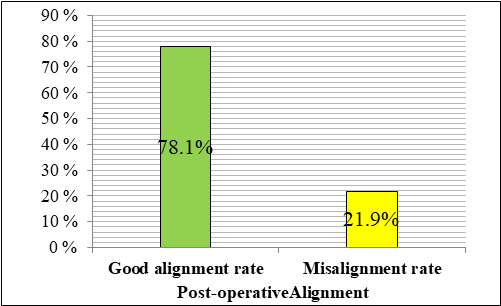
The postoperative outcome of the studied group was assessed according to the postoperative alignment which revealed that 50 patients had good alignment giving a rate of 78.1% while only 14 cases had misalignment in a rate of 21.9%, (Table 3.5 and Figure 3.4) .
Further analysis was performed to assess the effect of other variables and parameters on the postoperative outcome , cross tabulation was performed (Tabe3. 6), using the alignment status (misalignment or good alignment) as dependent variable against other variables as independent variables, result of this analyses revealed that these variables did not affect the final postoperative outcome of the patients, in all comparisons, P> value > 0.05. However, it is worth mentioning that type of surgery could have an effect on the outcome but did not reach the statistical significance, where all cases with misalignment managed with RR, and the P. value was (0.087) which is close to the significance cutoff value of 0.05.
Additionally, the mean degree of deviation was assessed across the postoperative alignment status and no significant difference had been found in the degree of deviation between cases with misalignment vs. those with good alignment, (Table .3. 7) .
Table3. 1. Age and gender distribution of the studied group.
Variable
No.
%
Age (year)
≤ 10
26
40.6
11 – 20
16
25.0
21 – 30
15
23.4
> 30
7
10.9
Total
64
100
Gender
Female
37
57.8
Male
27
42.2
Total
64
100
Figure 3.1.Gender distribution of the studied group with Female to Male ratio.
Table 3.2. Squint types and Presence of Amblyopia among the studied group
Squint type
No.
%
Constant
25
39.1
IE
23
35.9
AE
16
25.0
Total
64
100.0
Amblyopia
Positive
24
37.5
Negative
40
62.5
Total
64
100.0
IE : Intermittent Exotropia
AE: Alternative Exotropia
Figure3. 2. Type of surgery used in management of the 64 patients.
Figure3. 3. Distribution of the 64 patients according to the presence of refractive errors.
Table 3.3. Types of Refractive errors reported among the studied group (N = 64).
Refractive error
No.
%
Myopia
7
43.8
Hypermetropia
4
25.0
Myopia or hypermetropa with Astigmatism
5
31.2
Total
16
100.0
Table 3.4. Frequency distribution and descriptive statistics of degree of Vertical deviation of the studied group (N = 64).
Vertical deviation
No.
%
Positive
10
15.6
Negative
54
84.4
Total
64
100.0
Degree of deviation
Mean
35.8
-
-
SD*
11.7
-
-
Range
20 - 70
-
-
Median
35.0
-
-
IQR**
30 - 40
-
-
SD: standard deviation, IQR: inter-quartile range for the median
Table 3.5. Postoperative alignment status of the studied group, (N = 64).
Alignment
No.
%
Misalignment
14
21.9
Good alignment
50
78.1
Total
64
100.0
Figure3. 4. Post-operative alignment rates of the studied group (N = 64).
Table 3.6. Cross-tabulation for the relationship between post-operative alignment and other variables
Variable
Alignment
P. value
Misalignment
Good alignment
No.
%
No.
%
Age (year)
≤ 10
4
28.6
22
44.0
0.119
NS
11 - 20
3
21.4
13
26.0
21 - 30
3
21.4
12
24.0
> 30
4
28.6
3
6.0
Gender
Female
8
57.1
29
58.0
0.954
NS
Male
6
42.9
21
42.0
Squint type
Constant
4
28.6
21
42.0
0.216
NS
IE
4
28.6
19
38.0
AE
6
42.9
10
20.0
Amblyopia
Positive
5
35.7
19
38.0
0.876
NS
Negative
9
64.3
31
62.0
Type of surgery
RR
14
100.0
41
82.0
0.087
NS
BLR
0
0.0
9
18.0
Refractive error
Yes
3
21.4
13
26.0
0.727
NS
None
11
78.6
37
74.0
Vertical deviation
Positive
1
7.1
9
18.0
0.323
NS
Negative
13
92.9
41
82.0
Table3. 7. Comparison of mean degree of deviation across postoperative alignment .
Alignment
Number of patients
Degree of deviation
Mean
SD
Misalignment
14
35.71
9.972
Good alignment
50
35.86
12.224
P. value, (t test to compare means), = 0.968 NS
4. DISCUSSION
4.1. Overview:
Strabismus is an ophthalmic syndrome characterized by a deviation of the visual axis of one eye relative to the other. It may be constant or intermittent, concomitant or not, with primary or secondary sensory changes due to the deviation [5].
Strabismus has an expected predominance of 1%–3%. Exodeviation are more continuous in females than males and have a higher predominance in sunnier scopes, involving roughly 25% of the instances of strabismus in the Western world and 72% in Asia [6].
Treatment is indicated with increasing tropia phase to preserve or restore binocular function and restore/reconstruct normal ocular alignment. While medical treatment is sometimes helpful for temporary relief, surgical therapy is the preferred definitive treatment modality by most pediatric ophthalmologists and strabismologists [7].
It has long been recognized that exotropia tends to recur after strabismus surgery [8], accounting for its relatively low surgical success rate. Several studies have addressed the divergent post-operative drift after exotropia surgery, and have found that long-term post-operative alignment is better when there is over-correction in the very early period following procedures including bilateral lateral rectus recession, unilateral lateral rectus recession combined with medial rectus resection and various approaches using adjustable sutures. Initial over-correction also appears favorable in surgery for consecutive exotropia [9]. Studies found that long-term surgical results in exotropia are less encouraging when sensory status is added to the evaluation. Patients with anisometropia, lateral incomitance, and immediate postoperative undercorrection are at increased risk for poor outcomes and to require reoperations [10].
In the current study, a total of 64 cases with concomitant Exotropia who underwent surgical management were enrolled.
4.2. The postoperative outcome:
In the current study, majority of the patients; (55 /64 represented 85.9%), were managed with unilateral lateral rectus recession (RR) surgery while the remaining nine patients (14.1%) were managed with bilateral lateral rectus muscle recession (BLR).
In comparison to other studies, a different results observed in Mvogo et al study in 2007, in which they noticed that 80% of the patients had bilateral recession of the lateral recti and resection of the medial rectus of the more squinting eye under general anesthesia [5].
Another different results observed in Choi et al study in 2012, in which one hundred twenty-eight patients were included in this study. Fifty-five patients underwent BLR (43%), which was the highest proportion and 73 patients (57%), underwent RR [11].
Finally, Livir-Rallatos and colleagues in their study in 2002, that included Sixty-three patients had exodeviations from 35 Δ to 125 Δ and met the inclusion criteria of corrective surgery, in their study Fifty-two patients of them underwent bilateral lateral rectus recession (82%), and 11 patients of the remaining (18%) underwent unilateral recess/resect procedures [12].
The difference observed among studies can attributed to the sample size included in each study and due to the presence or lack of sufficiently specialized centers on one hand and other factors like poverty, lack of social security, fear and ignorance on the other hand.
In this study, the postoperative outcome of the studied group was assessed according to the postoperative alignment which revealed that 78.1% of patients had good alignment while only 21.9% of them had misalignment.
In comparison to other studies, a comparable results observed in Jung et al study in 2016, in which reported 39 adults with exotropia who underwent lateral rectus recession and medial rectus resection with initial over-correction <10 PD. Although 72% of patients achieved surgical success and only 10% had recurrence, 18% exhibited overcorrection, 64% continued to show consecutive esotropia at the final follow-up [13].
Differently, a study conducted by Lekskul and colleagues in 2018, in which postoperative orthoptic measurements revealed that 197 of 234 patients (84.19%) had successful surgical alignment, with total exodeviation <10 PD. 25 patients (10.68%) and 12 patients (5.13%) had postoperative exodeviation within 10–15 PD and >15 PD, respectively [14].
In accordance to Yang et al study in 2016, where 1228 patients studied, for patients classified as surgical successes, 712 (80.5%) were considered as demonstrating a postoperative surgical success, while 172 (19.5%) a surgical failure [15].
A lower results observed in a study done by Pineles and colleagues in 2010, in which of 197 patients identified, 50 were reevaluated. Results obtained showed that 64% had an excellent outcome, whereas the remaining patients achieved either a fair (18%) or a poor (18%) outcome. [16].
Several reasons could explain these differences. First, the sample size included in each study, inclusion of children as subjects in some studies may have contributed to increased postoperative recurrence of manifested exodeviation due to age-related deterioration in the fusional convergence mechanism. Moreover, other reported a lower success rate of bilateral LR recession, which was a preferred procedure for children in those studies, compared with combined medial rectus (MR) resection with LR recession procedures because of the tethering effect from MR resection [17]. Finally, follow-up period is an important factor, as short period of follow-up may lead to overestimate the successful surgical alignment.
Furthermore, in the current study analyses revealed that age, gender, sequent type, Amblyopia, type of surgery, Refractive error and Vertical deviation did not affect the final postoperative outcome of the patients, in all comparisons (P value > 0.05), meaning this finding could have an effect on the outcome but did not reach the statistical significance.
In comparison to other studies. A comparable results observed in a study conducted by Yang and colleagues in 2016, as found that factors such as sex, age at onset, age at surgery, duration of deviation, refractive errors, anisometropia, preoperative angle of exotropia, and surgical methods were not associated with surgical results obtained (P>0.05) (47).
Differently, Choi and their colleagues in their study in 2012, observed that no statistically significant difference in mean age at surgery, gender, Amblyopia, mean duration from onset of deviation to surgery, and follow-up period were observed between the groups (P>0.05), while a significant association observed in concern of preoperative angle of deviation, at both near and distant vision [11].
Differences in results obtained can explained by sample size enrolled in each study. Additionally, although relatively uniform manipulations for surgery and examination were followed in each hospital, the fact that many separate surgeons and examiners were used will introduce some variability in the data. Also, the follow-up times were quite variable among individual cases and the average follow-up time was somewhat brief for evaluating long-time therapeutic outcomes. Finally, even though exotropia onset was confirmed with photographic documentation in some patients, in many cases the onset of exotropia in this study was based on patient history, which can be subject to recall bias.
Several surgical approaches have been used successfully to treat exotropia. The choice of procedure classically has been based on the measured distance/near differences. Some authors have suggested that the patients with basic type primary exotropia should be treated with unilateral recess/resect procedure. However, for the surgical treatment of large-angle exotropia binocular surgery is the most commonly used approach involving three or four horizontal rectus muscles. This procedure is widely used because it avoids significant limitations of ocular movement, which could occur in surgeries of greater magnitude. In earlier publications, many ophthalmologists chose to operate on two horizontal muscles and correct residual deviations with second or third procedures with variable results [18].
Others, who were in the minority, considered simultaneous four horizontal muscle surgery to be a superior approach for these deviations. However, RR surgery has more advantages as it preserves some muscles if a repeat operation is required, avoiding the exposure of the dominant eye to the inherent risks of a surgical procedure and reducing surgical time [18].
4.3. Medical characteristics:
In the current study, refractive errors were documented in 16 patients, (25%), out of these 16 cases, seven patients presented with Myopia (43.8%), Four patients presented with hypermetropia (25%) and five cases (31.2%) had Myopia or hypermetropia with astigmatism. In the present study, frequency distribution of vertical deviation revealed that 10 cases (15.6%) had vertical deviation while 54 (84.4%) had not, on the other hand, the mean degree of deviation, was 35.8 ± 11.7 (range: 20 – 70) and a median of 35.
In comparison to other disease, different results observed in Mvogo et al study in 2007, in which of 41 patients underwent surgery, there were nine cases of amblyopia (22%), four cases of myopia (9.7%), 14 cases of hypermetropia (34%), 10 cases of hypermetropic astigmatism (42.3%), 10 cases of myopic astigmatism (42.3%) and three cases of mixed astigmatism (7.3%) [5].
4.4. General characteristics :
In the current study, Regarding the gender distribution, females were dominant (57.8%) females vs. (42.2%) males among the studied group, with a female to male ratio of 1.3:1, i.e. there was a slight female predominance, which was similarly observed in Gezer et al study in 2004, where female were (58.2%) and male patients (47.8%) [14]. On the contrary, Livir-Rallatos and collegues in their study in 2002, reported the clinical records of 63 patients out of which 33 were males and 30 were females [12].
Thus different studies showed slight variation in the gender distribution and this can be attributed to the fact that females are more concerned about their cosmetic appearance this seems to be a reason for more female patients undergoing surgery in our study.
Additionally, in this study, the age of the studied group ranged between 2-61 years with a median age of 14 years, majority of the cases, (89.1%), within the age of 30 years or less.
In comparison to other studies, ages of the patients in Saleem et al study in 2013 was ranged from 5 to 35 years (mean age 16.45 years, standard deviation ±7.42 years). In a similar study conducted by Jeoung JW and colleagues in 2006, the average age of the patients at the time of the surgery was less i.e., 7.8 ±5.9 years (mean ± standard deviation, ranging from 2 to 53 years) [19]. Furthermore, in a study conducted by Mvogo and colleagues in 2007, [5] the average age was 18.7 years ±11.2 that differed from our study. The high average age at the time of operation in some studies is because people hardly accept surgery in children, more so when it concerns the eyes. Moreover, the time lapse between the diagnosis and surgery is very important as it can aggravate the amplitude of the strabismus angle. In effect, patients who have witnessed operated cases are more motivated for surgery. The optimum age for surgery is when the child is able to undergo orthoptic assessment or when the functional and cosmetic symptoms become evident [20,21].
Conclusions and Recommendations
The results of this study are encouraging and show satisfactory ocular alignment 2.factors such as age, gender, preoperative visual acuity were not significant factors for favorable surgical outcome .
3.Strabismus surgery can help to preserve or restore the binocular vision.
5.2. Recomendation:
1.Further studies should be done for other outcomes such as improving stereopsis ,cosmetic or diplopia .
2.Larger number of patients with longitudinal follow up to assess more factors that affect the outcome .
Funding: No funding sources
Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee of Najaf Health Department, Al Furat Teaching Hospital
References
Bui Quoc, Emmanuel, and Chantal Milleret. "Origins of strabismus and loss of binocular vision." Frontiers in integrative neuroscience 8 (2014): 71.https://doi.org/10.3389/fnint.2014.00071
3.American Academy of Opthalmology. BCSC: Section 6, Pediatric Ophthalmology and Strabismus. United States: Published in collaboration with The European Board of Ophthalmology subcommittee; 2018-2019.
Mvogo, Côme Ebana, et al. "Surgical management of primary exotropia in Cameroon." Clinical Ophthalmology 1.4 (2007): 471-474. https://www.tandfonline.com/doi/full/10.2147/opth.s12160081
Govindan, Malu, et al. "Incidence and types of childhood exotropia: a population-based study." Ophthalmology 112.1 (2005): 104-108.https://doi.org/10.1016/j.ophtha.2004.07.033
Eibschitz-Tsimhoni, Maya, et al. "Current concepts in the management of concomitant exodeviations." Comprehensive Ophthalmology Update 8.4 (2007): 213-223.https://europepmc.org/article/med/17999835
Lee, Se-Youp, and Young Chun Lee. "Relationship between motor alignment at postoperative day 1 and at year 1 after symmetric and asymmetric surgery in intermittent exotropia." Japanese journal of ophthalmology 45.2 (2001): 167-171. https://doi.org/10.1016/S0021-5155(00)00351-8
Langmann, A., et al. "Dose-effect relation in surgery for consecutive exotropia in adults." Der Ophthalmologe 102 (2005): 869-872.DOIhttps://doi.org/10.1007/s00347-005-1210-x
Wu, Haixiang, et al. "Binocular status after surgery for constant and intermittent exotropia." American journal of ophthalmology 142.5 (2006): 822-826. https://www.sciencedirect.com/science/article/pii/S0002939406007707
Choi, Jin, et al. "The long-term survival analysis of bilateral lateral rectus recession versus unilateral recession-resection for intermittent exotropia." American journal of ophthalmology 153.2 (2012): 343-351. https://doi.org/10.1016/j.ajo.2011.06.024
Livir-Rallatos, Gerasimos, Kammi B. Gunton, and Joseph H. Calhoun. "Surgical results in large-angle exotropia." Journal of American Association for Pediatric Ophthalmology and Strabismus 6.2 (2002): 77-80. https://doi.org/10.1067/mpa.2002.122059
Jung, Eun Hye, Seong-Joon Kim, and Young Suk Yu. "Factors associated with surgical success in adult patients with exotropia." Journal of American Association for Pediatric Ophthalmology and Strabismus 20.6 (2016): 511-514.https://doi.org/10.1016/j.jaapos.2016.08.011
Lekskul, Apatsa, Tatha Supakitvilekarn, and Tanyatuth Padungkiatsagul. "Outcomes of undercorrection in surgical management and binocular vision gained of adult intermittent exotropia." Clinical Ophthalmology (2018): 1763-1767. https://www.tandfonline.com/doi/full/10.2147/OPTH.S174695
Yang, Min, et al. "Clinical characteristics and surgical outcomes in patients with intermittent exotropia: a large sample study in South China." Medicine 95.5 (2016): e2590. DOI: 10.1097/MD.0000000000002590
Pineles, Stacy L., et al. "Long-term results of the surgical management of intermittent exotropia." Journal of American Association for Pediatric Ophthalmology and Strabismus 14.4 (2010): 298-304.https://www.sciencedirect.com/science/article/pii/S1091853110003368
Kushner, Burton J. "Selective surgery for intermittent exotropia based on distance/near differences." Archives of Ophthalmology 116.3 (1998): 324-328. doi:10.1001/archopht.116.3.324
Saleem, Quratul Ain, et al. "Outcome of unilateral lateral rectus recession and medial rectus resection in primary exotropia." BMC research notes 6 (2013): 1-5.DOIhttps://doi.org/10.1186/1756-0500-6-257
Jeoung, Jin Wook, Min Joung Lee, and Jeong-Min Hwang. "Bilateral lateral rectus recession versus unilateral recess-resect procedure for exotropia with a dominant eye." American journal of ophthalmology 141.4 (2006): 683-688. https://www.sciencedirect.com/science/article/pii/S0002939405012249
Keenan, J. M., and H. E. Willshaw. "The outcome of strabismus surgery in childhood exotropia." Eye 8.6 (1994): 632-637.https://www.nature.com/articles/eye1994158
Stoller, Scott H., John W. Simon, and Lloyd L. Lininger. "Bilateral lateral rectus recession for exotropia: a survival analysis." Journal of Pediatric Ophthalmology & Strabismus 31.2 (1994): 89-92. https://doi.org/10.3928/0191-3913-19940301-06
Advertisement
Recommended Articles
Research Article
Epidemiological And Therapeutic Aspects of Spermatic Cord Torsion in The Pediatric Surgery Department of the mother and Child University Hospital of Libreville from January 2019 to October 2022
Nkole Aboughe Mélina,
...
Ondo Ndong F.
Published: 02/11/2025
Download PDF
Cite
x
APA
Mélina, N. A., Lapue C., C., Doussiemou S., I., E., C. & Ndong F., O. (2025). Epidemiological And Therapeutic Aspects of Spermatic Cord Torsion in The Pediatric Surgery Department of the mother and Child University Hospital of Libreville from January 2019 to October 2022. Himalayan Journal of Medicine and Surgery, 6(2), 1-3.
MLA
Mélina, Nkole Aboughe, et al. "Epidemiological And Therapeutic Aspects of Spermatic Cord Torsion in The Pediatric Surgery Department of the mother and Child University Hospital of Libreville from January 2019 to October 2022." Himalayan Journal of Medicine and Surgery 6.2 (2025): 1-3.
Chicago
Mélina, Nkole Aboughe, Chassem Lapue C., Ipouka Doussiemou S., Comlan E. and Ondo Ndong F.. "Epidemiological And Therapeutic Aspects of Spermatic Cord Torsion in The Pediatric Surgery Department of the mother and Child University Hospital of Libreville from January 2019 to October 2022." Himalayan Journal of Medicine and Surgery 6, no. 2 (2025): 1-3.
Harvard
Mélina, N. A., Lapue C., C., Doussiemou S., I., E., C. and Ndong F., O. (2025) 'Epidemiological And Therapeutic Aspects of Spermatic Cord Torsion in The Pediatric Surgery Department of the mother and Child University Hospital of Libreville from January 2019 to October 2022' Himalayan Journal of Medicine and Surgery 6(2), pp. 1-3.
Vancouver
Mélina NA, Lapue C. C, Doussiemou S. I, E. C, Ndong F. O. Epidemiological And Therapeutic Aspects of Spermatic Cord Torsion in The Pediatric Surgery Department of the mother and Child University Hospital of Libreville from January 2019 to October 2022. Himalayan Journal of Medicine and Surgery. 2025 Jul;6(2):1-3.
Download PDF
Case Report
Management of Urethral Prolapse in Girls at the Jeanne Ebori Foundation Mother-Child University Hospital: A Report of 7 Cases
Nkole Aboughe M.,
...
Ondo Ndong F.
Published: 25/10/2025
Download PDF
Cite
x
APA
Aboughe M., N., M., A., Lapue C., C., Nguéma J.H., N., E., C. & Ndong F., O. (2025). Management of Urethral Prolapse in Girls at the Jeanne Ebori Foundation Mother-Child University Hospital: A Report of 7 Cases. Himalayan Journal of Medicine and Surgery, 6(2), 1-3.
MLA
Aboughe M., Nkole, et al. "Management of Urethral Prolapse in Girls at the Jeanne Ebori Foundation Mother-Child University Hospital: A Report of 7 Cases." Himalayan Journal of Medicine and Surgery 6.2 (2025): 1-3.
Chicago
Aboughe M., Nkole, Abegue M., Chassem Lapue C., Nzue Nguéma J.H., Comlan E. and Ondo Ndong F.. "Management of Urethral Prolapse in Girls at the Jeanne Ebori Foundation Mother-Child University Hospital: A Report of 7 Cases." Himalayan Journal of Medicine and Surgery 6, no. 2 (2025): 1-3.
Harvard
Aboughe M., N., M., A., Lapue C., C., Nguéma J.H., N., E., C. and Ndong F., O. (2025) 'Management of Urethral Prolapse in Girls at the Jeanne Ebori Foundation Mother-Child University Hospital: A Report of 7 Cases' Himalayan Journal of Medicine and Surgery 6(2), pp. 1-3.
Vancouver
Aboughe M. N, M. A, Lapue C. C, Nguéma J.H. N, E. C, Ndong F. O. Management of Urethral Prolapse in Girls at the Jeanne Ebori Foundation Mother-Child University Hospital: A Report of 7 Cases. Himalayan Journal of Medicine and Surgery. 2025 Jul;6(2):1-3.
Download PDF
Research Article
Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India
Rahul Rai,
...
Tushar
Published: 05/04/2025
Download PDF
Cite
x
APA
Rai, R., Paul, D. & None, T. (2025). Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India. Himalayan Journal of Medicine and Surgery, 6(1), 1-3.
MLA
Rai, Rahul, Dharam Paul and Tushar . "Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India." Himalayan Journal of Medicine and Surgery 6.1 (2025): 1-3.
Chicago
Rai, Rahul, Dharam Paul and Tushar . "Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India." Himalayan Journal of Medicine and Surgery 6, no. 1 (2025): 1-3.
Harvard
Rai, R., Paul, D. and None, T. (2025) 'Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India' Himalayan Journal of Medicine and Surgery 6(1), pp. 1-3.
Vancouver
Rai R, Paul D, Tushar T. Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India. Himalayan Journal of Medicine and Surgery. 2025 Jan;6(1):1-3.
Download PDF
Research Article
A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla
Shivali Ranote,
...
Ashutosh
Published: 05/04/2025
Download PDF
Cite
x
APA
Ranote, S., Sharma, A. & None, A. (2024). A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla. Himalayan Journal of Medicine and Surgery, 5(1), 1-6.
MLA
Ranote, Shivali, Ajay Sharma and Ashutosh . "A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-6.
Chicago
Ranote, Shivali, Ajay Sharma and Ashutosh . "A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-6.
Harvard
Ranote, S., Sharma, A. and None, A. (2024) 'A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-6.
Vancouver
Ranote S, Sharma A, Ashutosh A. A Silent Threat: Cervical Cancer Awareness and Prevention Among Women in Shimla. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-6.
hassan, Z. Y. M., Salman, R. M., Shareef, M. D., Al-Ameedy, H. T. & Abdulkafi, A. Q. (2023). The outcome of surgical correction of concomitant exotropia, local experience. Himalayan Journal of Medicine and Surgery, 4(6), 1-13.
MLA
hassan, Zainab Y. M., et al. "The outcome of surgical correction of concomitant exotropia, local experience." Himalayan Journal of Medicine and Surgery 4.6 (2023): 1-13.
Chicago
hassan, Zainab Y. M., Rusel M. Salman, Maryam D. Shareef, Hashim T. Al-Ameedy and Ali Q. Abdulkafi. "The outcome of surgical correction of concomitant exotropia, local experience." Himalayan Journal of Medicine and Surgery 4, no. 6 (2023): 1-13.
Harvard
hassan, Z. Y. M., Salman, R. M., Shareef, M. D., Al-Ameedy, H. T. and Abdulkafi, A. Q. (2023) 'The outcome of surgical correction of concomitant exotropia, local experience' Himalayan Journal of Medicine and Surgery 4(6), pp. 1-13.
Vancouver
hassan ZYM, Salman RM, Shareef MD, Al-Ameedy HT, Abdulkafi AQ. The outcome of surgical correction of concomitant exotropia, local experience. Himalayan Journal of Medicine and Surgery. 2023 Iss;4(6):1-13.