The present study was carried out to compare neuro-cognitive correlates-Visual-Motor Functioning, Memory Functioning (Remote Memory, Recent Memory. Mental Balance, Attention and Concentration, Delayed Recall, Immediate Recall, Retention of Similar Pair, Retention of Dissimilar Pair, Visual Retention and Recognition) Visuo-Constructional Ability, Response Inhibition and Perceptual Acuity between individuals with Schizophrenia and Normal population. Out of 30 individuals, 20 belonged to Normal Population and 10 belonged to Clinical Population. Within the Clinical Population, 6 exhibited florid symptoms and 4 were in Partial Remission Phase of Schizophrenia.GHQ-28 was used to screen Normal Population and PANSS was used to screen positive and negative symptoms of Schizophrenia. Tools used in the present study were Bender Visual Motor Gestalt Test -I, PGI-Memory Scale, Clock Drawing Test, Stroop Test and Nahor-Benson Test. Statistical analysis revealed significant differences between Normal and Clinical Population in areas of memory functioning, Visuo-Constructional Ability and Perceptual Acuity. Significant differences existed between Florid and Partial Remission Groups in Recent Memory, Attention and Concentration, Delayed Recall, Immediate Recall, Visual Retention and Recognition.
Keywords
Schizophrenia
Florid Symptoms
Partial Remission
Visual-Motor Functioning
Memory Functioning
Visuo-Constructional Ability
INTRODUCTION
Schizophrenia is a disorder characterized by extreme oddities in perception, thinking, action, sense of self and manner of relating to others. The hallmark symptom of schizophrenia is a significant loss of contact with reality, referred to as psychosis. Schizophrenia spectrum and other psychotic disorders are characterized by the following abnormalities: delusions, hallucinations, disorganized thinking (speech), grossly disorganized or abnormal motor behavior (including catatonia) and negative symptoms.
Neurocognitive deficits are deficits in speed of processing, attention / vigilance, working memory, verbal memory, visual memory, reasoning and problem solving, social cognition. Cognitive deficits are present at onset of illness producing substantial impairment. Psychotic symptoms remit with treatment, but functional impairments remain stable over time.
Schizophrenia patients experience many problems with their neurocognitive functioning. While engaged in tasks of Working Memory, patients with schizophrenia show less prefrontal brain activity compared to healthy controls. Evidence suggests that patients with schizophrenia have problems with the active, functional allocation of attentional resources meaning that they are unable to attend well on demand.
Snellenberg, a research scientist in the division of translational imaging at NYSPI suggests that the Dorso- Lateral-Pre-Frontal Cortex is compromised in patients with Schizophrenia.
Visuospatial ability refers to a person’s ability to identify visual and spatial relationship among objects, to imagine objects and to make global shapes by locating small components. Evidence shows a medium to large effect of poor visuospatial memory and poor visuospatial ability in people with schizophrenia compared to people without schizophrenia.
Visual constructional ability, a non-verbal ability, which depends on the integration of several higher brain functions including perception, planning and motor coordination, is compromised in schizophrenia. Schizophrenics exhibit an inability or difficulty to build, assemble or draw objects. It may be caused by lesions in the parietal lobe.
Perceptual functions like visual processing and visual perceptual difficulties are frequently disrupted in schizophrenia. Visual integration deficits are seen in contrast, contour, form and motion processing in schizophrenia. Numerous examples of poor form processing in schizophrenia include deficits in object recognition, grouping, perceptual closure processing etc. In Edward’s study on Visual-Motor Perceptual Dysfunction among Positive and Negative Schizophrenia, the result shows a significant difference in Visual-Motor Perceptual Dysfunction between the two groups, proving that Negative Schizophrenia had more deficits than Positive Schizophrenia. Rotation was also seen more in Negative Schizophrenia than Positive Schizophrenia.
Bozikas [1] conducted a Clock Drawing Test in patients with Schizophrenia (2004) to compare CDT performance of patients with schizophrenia with that of normal controls. Qualitative analysis of the clocks that were drawn revealed specific errors in the schizophrenia group relating to frontal processes: difficulty placing numbers in the correct position, failure to indicate the minute targets, displacement of the minute hand from the minute number and failure to draw a longer minute hand.
Executive impairments have been found on tests assessing set-shifting abilities, selective attention and inhibition of inappropriate responses [2]. Elvevaag and colleagues conducted an encoding study in which subjects had to state whether the letter “A” was present in a word (shallow level) or make a decision as to whether the word represented a living thing or not (deep level). Preliminary results indicated that patients’ performance was worse than that of controls۔
MATERIALS AND METHODS
Participants
The present study consisted of 30 adults, out of whom 20 fell under Normal Control Group (Screened through GHQ-28), 6 fell in Florid Phase Category of Schizophrenia and the rest in Partial Remission Category of Schizophrenia (Screened through PANSS).
Procedure
Information Schedule and Informed Consent Forms were provided to the Normal Population. For the Psychiatric Population, necessary information for filling the information schedule was collected from the patients’ family members. The study was comparative in nature with a between-group design. Administration of the tools took around 1 to 1.5 hours. For each individual Test, specific instructions and required stationery was provided to the participants .30 data were collected. The 20 Normal Controls underwent screening with the help of GHQ = 28 and the 10 Clinical Patients underwent screening through PANSS to determine Florid Symptom phase and Partial Remission phase of Schizophrenia. All the data collected were properly scrutinized. Proper scoring was done according to the different scoring systems / keys available for the different Performance Tests used in the present study. After arranging all scores on excel sheets, statistical analysis was done by using SPSS (Version 16). Mean and Standard Deviation was calculated for the Normal group and the Clinical group. Mann- Whitney U test was calculated to determine whether any significant differences existed between Normal- Clinical group and Florid-Partial Remission group with respect to the study variables. Graphical representations of Mean and Standard Deviation were provided. Results were interpreted.
Measures
Detailed Information Schedule: For Normal Controls, it consisted of Name, Sex, Educational Qualification, Religion, Mother Tongue, Area of Residence, Type of Family, Number of Family Members and Approximate Family Income, Staying with Family, History of Physical and Mental Illness, Contact Number etc. For Individuals with Schizophrenia, it consisted of Name, Sex, Educational Qualification, Religion, Mother Tongue, Area of Residence, Type of Family, Number of Family Members, Approximate Family Income, Staying with Family, Chief Complaints, Diagnosis, Medication, Duration of Illness, Family history of Psychiatric Illness, Contact Number etc.
Bender Visual Motor Gestalt Test I
The Bender Visual Motor Gestalt Test (abbreviated as Bender Gestalt Test), originally developed in 1938 by child Psychiatrist Lauretta Bender, is a psychological test used by mental health professionals to assess visual – motor functioning, developmental disorders and Neurological impairments in children aged 3 years and older and adults. Various measures of Validity differ, up to max of r = 0.50. Scoring Reliability (rescoring) is estimated to 0.92. The total test scores are fairly normally distributed.
PGI – Memory Scale
PGI Memory Scale, constructed and standardized in 1977 and included in the Battery of Organic Dysfunction, provides a comprehensive and simple scale to measure verbal and non – verbal memories on the basis of neurological theory; very short term, short term and long-term memories on the basis of experimental evidences and remote, recent and immediate memories on the basis of clinical practice of evaluation of memory. Validity of PGI Memory scale was found to have a correlation of .71 with Boston Memory Scale and .85 with the Wechsler memory scale. Its test – retest reliability over a period of 1-week ranges from 0.69 to 0.85 for ten subtests 0.90 for the total test (test – retest and split half).
Clock Drawing Test
The Clock Drawing Test (CDT) is neuropsychological instrument that covers a wide range of cognitive functions, including selective and sustained attention, auditory comprehension, verbal working memory, numerical knowledge, visual memory and reconstruction, visuospatial abilities, on -demand motor execution (praxis) and executive function. Three studies determining inter-rater reliabilities of the CDT in elderly in Brazil were found: one scored the tests with Shulman's method, while the others compared the accuracy of scales (Mendez, Shulman and Sunderland; Sunderland, Shulman, Manos & Wu and Wolf-Klein) and determined the inter-rater reliability of CDT performance. The Shulman score had the highest correlation with the MMSE score (r =0.65, P < .01). The Shulman and Sunderland methods had significantly the largest areas under the receiver operating characteristic curve (0.82 and 0.81, respectively; P = 0.000). They also had the highest sensitivity (68.8% and 65.5%, respectively) and specificity (84.2% and 84.1%, respectively). The inter - rater correlation coefficients were high for all 3 clock scoring methods.
Stroop Color and Word Test
The Stroop Color and Word Test (SCWT) is a neuropsychological test extensively used to assess the ability to inhibit cognitive interference that occurs when the processing of a specific stimulus feature impedes the simultaneous processing of a second stimulus attribute, well-known as the Stroop Effect. The reliability of the Stroop Scores is highly consistent across different versions of the test. In all cases, experimenters have looked at test – retest reliabilities covering periods from 1 minute to 10 days. Jensen (1965) reported reliabilities of 0.88, 0.79 and 0.71 for the three raw scores. Golden reported reliabilities of 0.89, 0.84 and 0.73 (N = 450) for the Group version of the test and reliabilities of 0.86, 0.82 and 0.73 (N = 30) for the individual version. Reliabilities for subjects given both the individual and group form were 0.85, 0.81 and 0.69 (N = 60).
Nahor Benson Test
It consists of 8 cards. Out of these, five cards contain a design each and three cards contain the instructions to be followed, i.e., subjects are required to draw shapes of objects. Five designs are based on developmental pattern. Cards IV and V represent copying designs with depth. Pershad and Verma, have studied the screening capacity and clinical utility of the test and found that cases who were diagnosed having brain dysfunction reproduced and made the drawing more incorrect as compared to those having no brain dysfunction. Correlations of errors with PQ (Performance Quotient) and VQ (Verbal Quotient) were found to be 0.27 and 0.45 respectively.
General Health Questionnaire – 28 (GHQ – 28)
The GHQ – 28 was developed by Goldberg [3] as a screening tool to detect those likely to have or to be at the risk of developing psychiatric disorders. It is a 28-item measure of emotional distress in medical settings. Test – retest reliability has been reported to be high (0.78 – 0.9) and inter – rater and Intra – rater reliability has been both shown to be excellent (Cronbach’s α = 0.9 – 0.95). High Internal Consistency has also been reported.
Positive and Negative Syndrome Scale (PANSS)
Published in 1987 by Stanley Kay, Lewis Opler and Abraham Fiszbein, the PANSS is known as the “Golden Standard” that all assessments of psychotic behavioral disorder should follow. It is a valid instrument used for the assessment of severity of schizophrenia symptoms. Test – retest Reliability for the total score and subscales is reported as 0.77 – 0.89.
RESULTS AND DISCUSSION
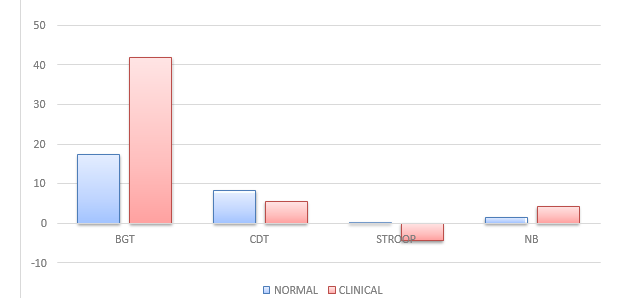
Table 1 is Showing Mean, Standard Deviation, Mann – Whitney U Values between Control and Clinical Group with respect to Visual – Motor Functioning (Bender Gestalt Test-1), Visuo – Constructional Ability (Clock Drawing Test), Response Inhibition (Stroop Test) and Perceptual Acuity (Nahor-Benson Test).
In the present study, the Clinical Population showed significant difficulties and inconsistencies in their performances on the dimensions of Visual-Motor Functioning, Visuo-Constructional Ability, Response Inhibition and Perceptual Acuity which may be attributed to severe symptom presentation (example Hallucinations) while taking the tests.
Evidence on studies of Visual-Motor functioning revealed significant differences in performance of schizophrenics, Goldberg’s study on Performance of Schizophrenics and Normal on BGT [3] showed that emotional factors seem to have an effect on the BG score; the Schizophrenics needed a significantly longer time to copy the figures than the Normal Controls.
Ransing, Khairkar, Mishra and Sakekar in the Journal of Neuropsychiatry and Clinical Neurosciences provided evidence about significantly poor performance of patients of Schizophrenia compared with healthy controls. Hermann and Morris conducted a study using 24 Schizophrenics with 24 healthy age- matched controls on Clock Drawing and found that patients with Schizophrenia performed significantly worse on Clock Drawing and copying.
Golden found significant differences between normal control group and psychiatric patients on all basic Stroop Color and Word Test measures. However, the degree of difference was greater on the Color - Word measure than on the Color and Word pages. The average interference measure for the normal patients was 0.00 (the expected average) while the psychiatric patients averaged (-6.1).
Schizophrenic patients were impaired significantly in detection of images that required grouping of stimulus
Table 1: Mann – Whitney U Values between Control and Clinical Group with respect to Visual-Motor Functioning, Visuo-Constructional Ability, Response Inhibition and Perceptual Acuity
Dimensions
Groups
Mean
Standard Deviation
Mann – Whitney U
Significance Level
Visual-Motor Functioning
Normal
Clinical
17.37
41.80
23.72
27.36
31
(0.002)
**
Visuo-Constructional Ability
Normal
Clinical
8.17
5.50
2.56
2.877
8.000
(0.000)
**
Response Inhibition
Normal
Clinical
0.12
-4.30
8.798
4.185
56.000
(0.56)
**
Perceptual Acuity
Normal
Clinical
1.40
4.20
2.343
2.150
0.000 (0.000)
**
*p=<0.05 level **p=<0.01 level
Figure 1: Graph showing Mean values of Normal and Clinical Group
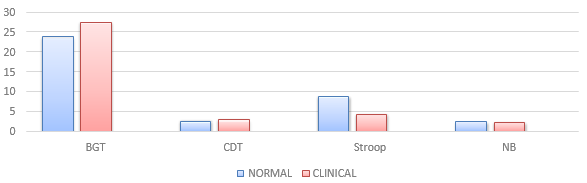
Figure 2: Graph Showing Standard Deviation Values of Normal and Clinical Group
Table 2: Showing Mean, Standard Deviation, Mann –Whitney U Values between Control and Clinical Group with respect to Memory Functioning and its Subdomains
Dimensions
Groups
Mean
Standard Deviation
Mann–Whitney U
Significance Level
Remote Memory
Normal
Clinical
4.47
2.60
1.63
1.265
4.5
(0.000)
**
Recent Memory
Normal
Clinical
3.73
2.50
1.31
1.509
30
(0.001)
**
Mental Balance
Normal
Clinical
7.47
5.80
1.87
2.10
17
(0.000)
**
Attention and Concentration
Normal
Clinical
10.33
7.50
2.44
2.068
0.00
(0.000)
**
Delayed Recall
Normal
Clinical
7.90
4.50
3.1
3.408
0.000
(0.000)
**
Immediate Recall
Normal
Clinical
8.13
4.60
3.01
1.897
4.5
(0.000)
**
Retention of Similar Pairs
Normal
Clinical
4.63
3.90
0.71
0.876
30
(0.001)
**
*p=<0.05 level **p=<0.01 level
elements into coherent object representations. This deficit was accompanied by longer reaction time in schizophrenic patients.
Figure 1 is graphical representation of mean values of normal and clinical group with respect to Visual–Motor Functioning (Bender Gestalt Test - 1) Visuo– Constructional Ability (Clock Drawing Test), Response Inhibition (Stroop Test) and Perceptual Activity (Nahor Benson Test).
Figure 2 is graphical representation of standard deviation values of normal and clinical groups with respect to Visual–Motor Functioning (Bender Gestalt Test-1), Visuo – Constructional Ability (Clock Drawing Test), Response Inhibition (Stroop Test) and Perceptual Acuity (Nahor Benson Test).
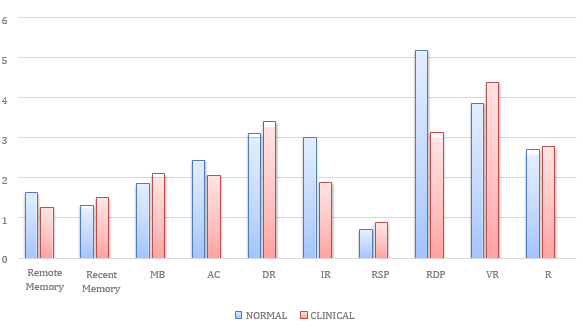
Table 2 is showing Mean, Standard Deviation, Mann –Whitney U Values between Control and Clinical Group with respect to Memory Functioning and its Sub – Domains (Remote Memory, Recent Memory, Mental Balance, Attention and Concentration, Delayed Recall, Immediate Recall, Retention of Similar Pair, Retention of Dissimilar Pair, Visual Retention and Recognition).
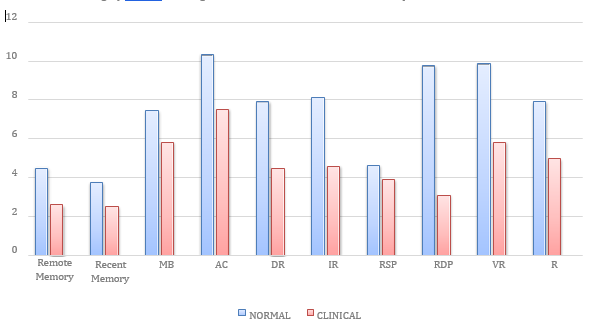
The Clinical Group showed greater deficits on all the sub-domains of Memory Functioning than their healthy counterparts. Saykin et al reported generalized impairment with more pronounced impairment in verbal learning, memory, visual-motor processing, attention, vigilance. On memory tests, patients were as impaired on tests of Immediate Recall as they were on tests on Delayed Recall. Paulsen et al suggested that memory difficulties found in patients with schizophrenics are primarily caused by deficits in encoding and retrieval rather than storage. Krishnadas compared 25 Schizophrenic patients with 25 Normal Controls and found that patients with Schizophrenia showed significant deficits on tests of Attention, Concentration, Visual, Verbal Memory, as compared to Normal Controls.
Figure 3: Graph Showing Mean Values of Normal and Clinical Group
Fig 4: Graph Showing SD Values of Normal and Clinical Group
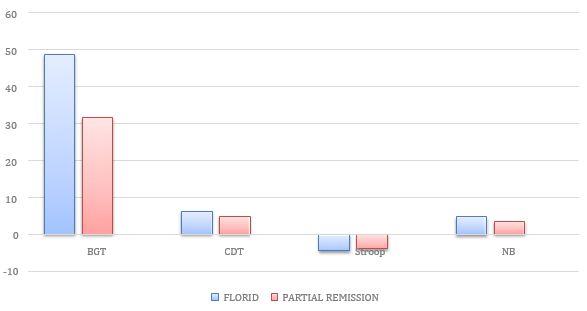
Figure 5: Graph Showing Mean Values of Florid and Partial Remission Group of Schizophrenia
Figure 6: Graph Showing SD values of Florid and Partial Remission Group of Schizophrenia
Table 3: Values between florid and remission groups of clinical groups with respect to visual–motor functioning, visuo–constructional ability, response inhibition and perceptual acuity
Dimensions
Groups
Mean
Standard Deviation
Mann–Whitney U
Sig. Level
Visual-Motor Functioning
Florid
Partial Remission
48.76
31.50
26.097
29.592
8.000
(0.476)
-
Visuo-Constructional Ability
Florid
Partial Remission
6.00
4.75
3.033
2.872
8.50 (0.476)
-
Response
Inhibition
Florid
Partial Remission
-4.52
-3.96
5.235
2.573
10
(0.762)
-
*p=<0.05 level **p=<0.01 level
Table 3 is showing mean, standard deviation, Mann – Whitney U values between florid and remission groups of clinical groups with respect to Visual – Motor Functioning (Bender Gestalt Test-1), Visuo– Constructional Ability (Clock Drawing Test), Response Inhibition (Stroop Test) and Perceptual Acuity (Nahor Benson).
Figure 3 is graphical representation of mean values of Normal and Clinical Group with respect to Remote Memory, Recent Memory, Mental Balance, Attention and Concentration, Delayed Recall, Immediate Recall, Retention of Similar Pair, Retention of Dissimilar Pair, Visual Retention and Recognition domains of Memory Functioning.
Figure 4 is graphical representation of standard deviation values of normal and clinical group with respect to remote memory, recent memory, mental balance, attention and concentration, delayed recall, immediate recall, retention of similar pair, retention of dissimilar pair, visual retention and recognition domains of memory functioning.
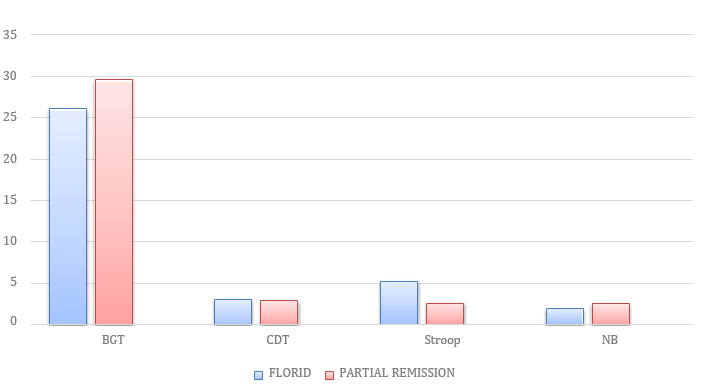
In the present study, greater deficits were observed for Florid Group than the Partial Remission Group on the dimensions of Visual-Motor Functioning, Visuo-Constructional Ability, Response Inhibition and Perceptual Acuity owing to severe symptom presentation where some of the clinical patients in the Florid Phase were hallucinating at the time of test administration.
Table 4: Mean, Standard Deviation, Mann–Whitney U Values between Florid and Remission Groups of Clinical Group with respect to Visual–Motor Functioning, Visuo–Constructional Ability, Response Inhibition and Perceptual Acuity
Dimensions
Groups
Mean
Standard
Deviation
Mann–Whitney U
Sig. Level
Visual-Motor Functioning
Florid
Partial Remission
48.76
31.50
26.097
29.592
8.000
(0.476)
-
Visuo-Constructional Ability
Florid
Partial Remission
6.00
4.75
3.033
2.872
8.50
(0.476)
-
Response Inhibition
Florid
Partial Remission
-4.52
-3.96
5.235
2.573
10
(0.762)
-
*p=<0.05 level **p=<0.01 level
For the dimension of Visual-Motor Functioning, supporting evidence have been provided by Green and Walker [4] in the Journal of Abnormal Psychology who reported that negative symptoms ratings were inversely proportional with performance on Visual-Motor function tasks, whereas positive symptoms were inversely associated with verbal memory performances.
Studies concerning CDT revealed that Positive symptoms affect CDT outcomes more than negative symptoms.
Everett, Laplante and Thomas concluded that the schizophrenic patients’ deficits on the Stroop Test appeared to be related to cognitive fatigue.
People with non-remitted Schizophrenia were shown to have significant impairments on Visuo-Spatial ability [5].
Table 4 showing mean, standard deviation, Mann–Whitney U values between florid and remission groups of clinical groups with respect to visual–motor functioning (bender gestalt test-1), visuo–constructional ability (clock drawing test), response inhibition (Stroop test) and perceptual acuity (Nahor Benson).
In the present study, greater deficits were observed for Florid Group than the Partial Remission Group on the dimensions of Visual-Motor Functioning, Visuo-Constructional Ability, Response Inhibition and Perceptual Acuity owing to severe symptom presentation where some of the clinical patients in the Florid Phase were hallucinating at the time of test administration.
For the dimension of Visual-Motor Functioning, supporting evidence have been provided by Green and Walker [4] in the Journal of Abnormal Psychology who reported that negative symptoms ratings were inversely proportional with performance on Visual-Motor function tasks, whereas positive symptoms were inversely associated with verbal memory performances.
Though evidence shows greater deficits in BGT performance under the influence of negative symptoms of Schizophrenia, in the present study no significant differences were observed between Florid and Partial Remission Group of Schizophrenia owing to subjects’ non-cooperativeness to perform the Bender Gestalt Test1. No significant differences were found to exist between the Florid Group and Partial Remission group on the dimensions of Visuo-Constructional Ability, Response Inhibition and Perceptual Acuity owing to severe symptom presentation in the Florid Symptom Group and non – cooperativeness to perform the test by the partially remitted group of Schizophrenia.
Figure 5 is the graphical representation of Mean values of Florid and Partial Remission Group of Schizophrenia with respect to Visual – Motor Functioning (Bender Gestalt Test-1), Visuo – Constructional Ability (Clock Drawing Test), Response Inhibition (Stroop Test) and Perceptual Acuity (Nahor Benson).
Figure 6 is graphical representation of Standard Deviation values of Florid and Partial Remission Group of Schizophrenia with respect to Visual–Motor Functioning (BGT-1), Visuo–Constructional Ability (CDT), Response Inhibition (Stroop Test) and Perceptual Acuity (Nahor Benson).
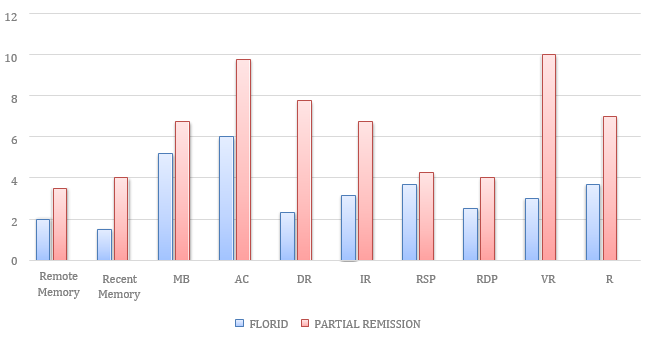
Within the Clinical population, individuals exhibiting Florid Symptoms of Schizophrenia displayed greater deficits in all the ten sub-domains than the partially
Table 5: Values between Florid and Remission Groups of Clinical Group with respect to Memory Functioning along with its sub-domains
Dimensions
Groups
Mean
Standard Deviation
Mann–Whitney U
Sig. Level
Remote Memory
Florid
Partial Remission
2.00
3.50
1.265
0.577
4.000 (0.114)
Recent Memory
Florid
Partial Remission
1.50
4.00
0.837
0.816
0.50 (0.01)
**
Mental Balance
Florid
Partial Remission
5.17
6.75
2.563
0.500
4.50 (0.114)
Attention and Concentration
Florid
Partial Remission
6.00
9.75
0.894
0.500
0.000 (0.01)
**
Delayed Recall
Florid
Partial Remission
2.33
7.75
2.582
0.500
0.000 (0.01)
**
Immediate Recall
Florid
Partial Remission
3.17
6.75
0.408
0.500
0.000 (0.01)
**
Retention of Similar Pairs
Florid
Partial Remission
3.67
4.25
1.033
0.500
7.000 (0.352)
Retention of Dissimilar Pairs
Florid
Partial Remission
2.50
4.00
2.739
4.596
9.000 (0.610)
Visual Retention
Florid
Partial Remission
3.00
10.00
3.286
0.816
0.000 (0.01)
**
Recognition
Florid
Partial Remission
3.67
7.00
2.875
0.816
1.000 (0.018)
**
*p=<0.05 level **p=<0.01 level
remitted individuals. Talreja Shah and Kataria found that 70% of Schizophrenics were found to have cognitive dysfunctions for attention, concentration, memory, language and executive functioning and Positive symptoms were associated with memory (p<0.001) and attention impairment (p<0.05).
Significant differences were found to exist between Florid and Partial Remission Group on Recent Memory, Attention and Concentration, Delayed Recall, Immediate Recall, Visual Retention and Recognition. Patients with Schizophrenia (in Remission) showed significant deficits on tests of Attention, Concentration, Verbal and Visual Memory. They fared worse on almost all the battery of
Figure 7: Graph Showing Mean Values of Florid and Partial Remission Group of Schizophrenia
Figure 8: Graph Showing SD Values of Florid and Partial Remission Group of Schizophrenia
Cognitive Tests administered to them, compared to Normal Controls [6]. Deficits in Attention and Information Processing in Schizophrenia contribute to deficits in Executive Functioning and Working Memory. Specific deficit in Verbal Memory could be attributed to an aberration in the automatic speed of activation in semantic networks which may be mediating the thought disorder.
No significant differences occurred between Florid and Partial Remission Group on the dimensions of tests of Remote Memory, Mental Balance, Retention of Similar Pairs and Retention of Dissimilar Pairs.
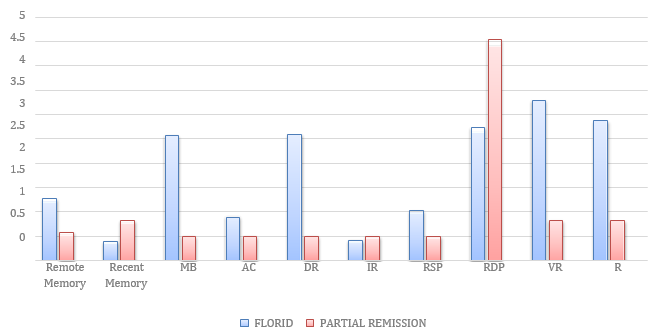
Figure 7 is graphical representation of mean values of florid and partial remission group of schizophrenia with respect to remote memory, recent memory, mental balance, attention and concentration, delayed recall, immediate recall, retention of similar pair, retention of dissimilar pair, visual retention and recognition domains of memory functioning.
Graphical representation of standard deviation values of florid and partial remission group of schizophrenia with respect to remote memory, recent memory, mental balance, attention and concentration, delayed recall, immediate recall, retention of similar pair, retention of dissimilar pair, visual retention and recognition domains of memory functioning.
CONCLUSION
In conclusion, the results of the present study suggest significant association of neurocognitive deficits especially abnormalities in visual-motor functioning, memory functioning, executive functioning, visual- constructional abilities in persons with Schizophrenia. Greater deficiencies were exhibited by schizophrenics who were in Partial Remission Phase.
Although interesting findings have been obtained from the present study, certain limitations such as limited sample size, time constraint and limited age range of participants were present.
Cognitive deficits are useful in identifying individuals who are at risk for the disease. They may serve as early predictors of the illness. They have helped in monitoring the clinical course of the illness, in influencing the outcome of treatment. The cognitive deficits are more directly related to functional outcome than symptoms are. Therefore, improving cognitive functioning would improve the quality of life of patients and would necessitate less dependence on psychiatric care and fewer hospital admissions.
Future work should obtain a larger sample size; consider gender differences which would yield more benefits and more verifiable conclusions. Cognitive impairments in other types of psychotic disorders like Mood Disorders (Major Depression, Bipolar Disorders) can be explored and compared with the cognitive deficits in Schizophrenia. How Cognitive deficits contribute to limitations in Planning, goal-directed behavior and Insight in Schizophrenia-this area is essential for further consideration.
REFERENCE
Bozikas, V.P. "Clock drawing test in patients with schizophrenia." Psychiatry Research, vol. 121, no. 3, 2004, pp. 229–38.
Kalkstein, Solomon, I.H. "Neurocognition in schizophrenia." Behavioral Neurobiology of Schizophrenia and Its Treatment, 21 Apr. 2010, pp. 373–90.
Goldberg, F. "The performance of schizophrenic, retarded and normal children on the Bender Gestalt test." American Journal of Mental Deficiency, vol. 61, 1957, pp. 548–55.
Green, M., E.W. "Neuropsychological performance and positive and negative symptoms in schizophrenia." Journal of Abnormal Psychology, vol. 94, no. 4, 1985, pp. 460–69.
Lepage, M.M.B. "Neurocognition: Clinical and functional outcomes in schizophrenia." Canadian Journal of Psychiatry, vol. 59, no. 1, 2014, pp. 5–12.
Krishnadas, Rajeev, B.P. "Relationship of cognitive function in patients with schizophrenia in remission to disability: A cross-sectional study in an Indian sample." Annals of General Psychiatry, vol. 6, 2007, p. 19.
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Applied Medical Sciences and Research open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Recommended Articles
Research Article
Digital Implantology: Current Concepts, Clinical Applications, Limitations and Future Directions - A Narrative Review
Anukrity Chandra
Published: 30/07/2026
Download PDF
Cite
x
APA
Chandra, A. (2026). Digital Implantology: Current Concepts, Clinical Applications, Limitations and Future Directions - A Narrative Review. Himalayan Journal of Applied Medical Sciences and Research, 7(2), 1-7.
MLA
Chandra, Anukrity. "Digital Implantology: Current Concepts, Clinical Applications, Limitations and Future Directions - A Narrative Review." Himalayan Journal of Applied Medical Sciences and Research 7.2 (2026): 1-7.
Chicago
Chandra, Anukrity. "Digital Implantology: Current Concepts, Clinical Applications, Limitations and Future Directions - A Narrative Review." Himalayan Journal of Applied Medical Sciences and Research 7, no. 2 (2026): 1-7.
Harvard
Chandra, A. (2026) 'Digital Implantology: Current Concepts, Clinical Applications, Limitations and Future Directions - A Narrative Review' Himalayan Journal of Applied Medical Sciences and Research 7(2), pp. 1-7.
Vancouver
Chandra A. Digital Implantology: Current Concepts, Clinical Applications, Limitations and Future Directions - A Narrative Review. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jul;7(2):1-7.
Download PDF
Research Article
Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19
Aynar Talib Samad,
Yossra Saleh Khudhur
Published: 27/07/2021
Download PDF
Cite
x
APA
Talib Samad, A. & Khudhur, Y. S. (2021). Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19. Himalayan Journal of Applied Medical Sciences and Research, 2(2), 1-6.
MLA
Talib Samad, Aynar and Yossra Saleh Khudhur. "Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19." Himalayan Journal of Applied Medical Sciences and Research 2.2 (2021): 1-6.
Chicago
Talib Samad, Aynar and Yossra Saleh Khudhur. "Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19." Himalayan Journal of Applied Medical Sciences and Research 2, no. 2 (2021): 1-6.
Harvard
Talib Samad, A. and Khudhur, Y. S. (2021) 'Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19' Himalayan Journal of Applied Medical Sciences and Research 2(2), pp. 1-6.
Vancouver
Talib Samad A, Khudhur YS. Study of the Role of Serum Interleukin-6 in Inflammation among Pregnant Women with COVID-19. Himalayan Journal of Applied Medical Sciences and Research. 2021 Jul;2(2):1-6.
Download PDF
Research Article
Evalution CD11b, CD4, IL-17A and IL-23 as Biomarkers Immunological in Patients with Behçet’s Disease
Layla Saleh Abdul-Hassan,
...
Saeed hilal khudhair
Published: 13/07/2026
Download PDF
Cite
x
APA
Abdul-Hassan, L. S., Fadel, R. H. & khudhair, S. H. (2026). Evalution CD11b, CD4, IL-17A and IL-23 as Biomarkers Immunological in Patients with Behçet’s Disease. Himalayan Journal of Applied Medical Sciences and Research, 7(2), 1-7.
MLA
Abdul-Hassan, Layla S., Radhia H. Fadel and Saeed H. khudhair. "Evalution CD11b, CD4, IL-17A and IL-23 as Biomarkers Immunological in Patients with Behçet’s Disease." Himalayan Journal of Applied Medical Sciences and Research 7.2 (2026): 1-7.
Chicago
Abdul-Hassan, Layla S., Radhia H. Fadel and Saeed H. khudhair. "Evalution CD11b, CD4, IL-17A and IL-23 as Biomarkers Immunological in Patients with Behçet’s Disease." Himalayan Journal of Applied Medical Sciences and Research 7, no. 2 (2026): 1-7.
Harvard
Abdul-Hassan, L. S., Fadel, R. H. and khudhair, S. H. (2026) 'Evalution CD11b, CD4, IL-17A and IL-23 as Biomarkers Immunological in Patients with Behçet’s Disease' Himalayan Journal of Applied Medical Sciences and Research 7(2), pp. 1-7.
Vancouver
Abdul-Hassan LS, Fadel RH, khudhair SH. Evalution CD11b, CD4, IL-17A and IL-23 as Biomarkers Immunological in Patients with Behçet’s Disease. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jul;7(2):1-7.
Download PDF
Research Article
Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community
Vishal Dhatwalia,
Swati Chandel
Published: 10/12/2024
Download PDF
Cite
x
APA
Dhatwalia, V. & Chandel, S. (2024). Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research, 5(2), 1-5.
MLA
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5.2 (2024): 1-5.
Chicago
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5, no. 2 (2024): 1-5.
Harvard
Dhatwalia, V. and Chandel, S. (2024) 'Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community' Himalayan Journal of Applied Medical Sciences and Research 5(2), pp. 1-5.
Vancouver
Dhatwalia V, Chandel S. Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research. 2024 Jul;5(2):1-5.
Sarkar, S. & Datta, D. (2021). A Comparative Study of Neuro-Cognitive Correlates in Schizophrenia (Florid and Partial Remission Phase) and Normal Controls. Himalayan Journal of Applied Medical Sciences and Research, 2(2), 1-8.
MLA
Sarkar, Srinanda and Dr.Soheli Datta. "A Comparative Study of Neuro-Cognitive Correlates in Schizophrenia (Florid and Partial Remission Phase) and Normal Controls." Himalayan Journal of Applied Medical Sciences and Research 2.2 (2021): 1-8.
Chicago
Sarkar, Srinanda and Dr.Soheli Datta. "A Comparative Study of Neuro-Cognitive Correlates in Schizophrenia (Florid and Partial Remission Phase) and Normal Controls." Himalayan Journal of Applied Medical Sciences and Research 2, no. 2 (2021): 1-8.
Harvard
Sarkar, S. and Datta, D. (2021) 'A Comparative Study of Neuro-Cognitive Correlates in Schizophrenia (Florid and Partial Remission Phase) and Normal Controls' Himalayan Journal of Applied Medical Sciences and Research 2(2), pp. 1-8.
Vancouver
Sarkar S, Datta D. A Comparative Study of Neuro-Cognitive Correlates in Schizophrenia (Florid and Partial Remission Phase) and Normal Controls. Himalayan Journal of Applied Medical Sciences and Research. 2021 Jul;2(2):1-8.