The assessment of craniofacial dimension is not a new skill in orthodontics. Cephalometry is used to assess craniofacial growth and determine treatment responses. Cephalometric radiology was introduced in orthodontics during the 1930’s but the method really gained wider acceptance for practical application during the last 20 years [1]. Over the years, whole range of analysis has been developed by number of authors. The analysis will only supply answers to a particular set of questions and these answers will depend on correct application of the method and interpretation of results.
The successful treatment of orthodontics of orthognathic surgical treatment is dependent on careful diagnosis. It is important for the clinician to be able to predict the soft tissue changes resulting from alterations of the hard tissue. Many studies have attempted to evaluate the relationship between hard tissue surgery and the effects it has on the overlying soft tissue [2]. Though cephalometric analysis has its limitations, it is a tool which will guide us in planning orthodontic treatment.
The various cephalometric analysis given by many authors such as Cephalometric Analysis for Orthognathic Surgery (COGS) [3], Quadrilateral Analysis [4], Arnett Analysis [5], Burstone and Legan Soft Tissue Cephalometric Analysis [6], etc., were used for surgical patients for interpretation of results. All these analyses were based on hard tissue references with the paradigm shift to soft tissue. Arnett and Bergman [5], presented the facial keys to orthodontic diagnosis and treatment planning.
Widely used cephalometric analysis for surgical analysis of an orthognathic surgery case are
Burstone’s Cephalometric Analysis for Orthognathic Surgery (COGS)
DiPaolo’s Quadrilateral Analysis
Arnett’s Soft Tissue Cephalometric Analysis (STCA
Though each analysis has its own merits and demerits, there are many overlapping parameters studied by these three authors. Hence, the aim of the present study is to identify the significant parameters and overlapping parameters from the above analyses and to arrive at a CCAOS.
Obtaining The Lateral Cephalometric Radiograph
Lundstrom and Lundstrom [7] findings indicate that a horizontal line, related to natural head position, adjusted to natural head orientation when indicated, presents the most reliable basis for cephalometric analysis. Some patients assume an “Unnatural head position”. Accordingly, these patients need adjustment to “natural head orientation” [5].
Anatomical Landmarks Used for the Analysis
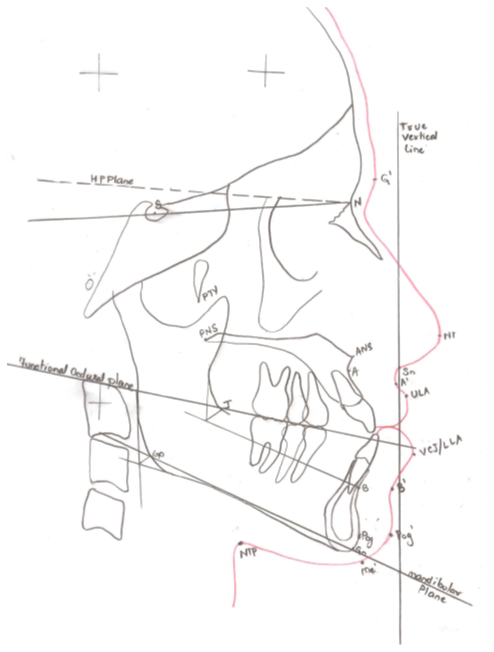
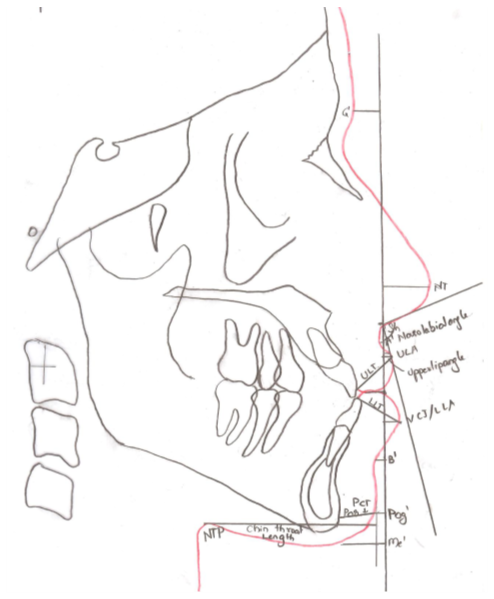
The landmarks used in the cephalometric analysis are the following (Figure 1).
Hard Tissues
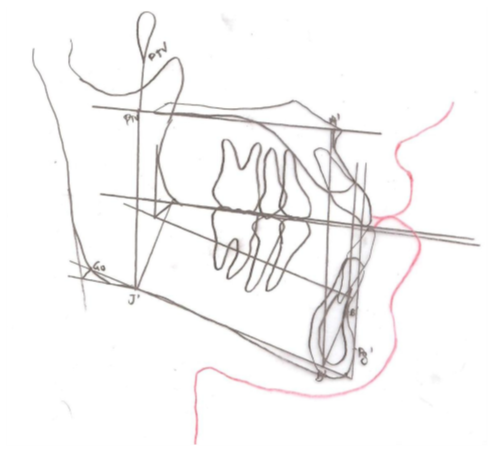
Sella (S), Nasion (N), Pterygomaxillary fissure (PTM), Subspinale (A), Supramentale (B), Pogonion (Pog), Anterior nasal spine (ANS), Posterior Nasal Spine (PNS), Gnathion (Gn), Gonion (Go) [3], J point, Nasal floor [4].
Soft Tissues
Glabella (G’), Nasal Tip (NT), Subnasale (Sn), Subspinale (A’), Submentale (B’), Upper Lip Anterior (ULA), Lower Lip Anterior (LLA), Pogonion (Pog’) [5].
Reference Planes
COGS [3]- Hard tissue-horizontal plane (H-P) [Surrogate Frankfurt Horizontal plane].
STCA [5] - Soft tissue –True vertical line.
Other Planes
Palatal plane- ANS-PNS [4], Mandibular Plane (MP)- GoGn [3,4] and Functional Occlusal Plane [3].